
![]()
Fourth Cranial Nerve Lesions
Cranial nerve IV is also known as the Trochlear nerve.
It is a purely motor nerve.
Isolated lesions of the trochlear nerve are very rare.
It is more commonly associated with third cranial nerve lesions.
Anatomy
Course of the Trochlear Nerve
- Originates in the trochlear nucleus, in the ventral midbrain.
- Nerves cross (decussate) around the aqueduct to the contralateral side of the brainstem prior to exiting.
- Each superior oblique muscle is supplied by fibres from the trochlear nucleus of the opposite side.
- Exits the brainstem on the dorsal surface of the midbrain, below the inferior colliculus.
- The only cranial nerve to exit dorsally.
- Curves around the cerebral peduncle, runs forward in the lateral wall of the cavernous sinus, between:
- Oculomotor nerve (above)
- Ophthalmic nerve (below)
- Enters the orbit via the superior orbital fissure (external to the common tendinous ring), passing:
- Below the frontal nerve
- Above the superior ramus of the oculomotor nerve
- Within the orbit, travels medially and diagonally across and above the levator palpebrae superioris and superior rectus, to innervate the superior oblique muscle.
Trochlear Nerve Innervations
| Function | Structure Innervated |
|---|---|
| Motor | Superior oblique muscle |
Pathology
Causes of a fourth cranial nerve lesion include:
- Demyelinating disease
- Multiple sclerosis
- Vascular disease
- Brainstem microvascular strokes
- Space-occupying lesions
- Tumours
- Aneurysms
- Abscesses
- Raised intracranial pressure
- Venoms
- Snake bite
- Thiamine deficiency
- Wernicke’s encephalopathy (as part of ophthalmoplegia)
- Trauma
- Skull base trauma
- Mononeuritis
- Diabetes
- Toxins
- Microvascular disease
- Paraneoplastic disease
- Connective tissue disease
- Infections (HIV, Lyme disease, syphilis)
- Idiopathic
- No clear cause found in some cases
- Rarely
- Cavernous sinus thrombosis
Clinical Assessment
Important Points of History
- Presenting problem usually diplopia.
- If headache present, raises suspicion for:
- Cerebral aneurysm (acute bleed or expansion)
- Intracranial tumour
- Raised intracranial pressure
Important Points of Examination
- Strabismus
- May be an obvious squint of the affected eye.
- Head tilt
- Patient may tilt head away from the lesion (towards the opposite shoulder) in an attempt to maintain binocular vision.
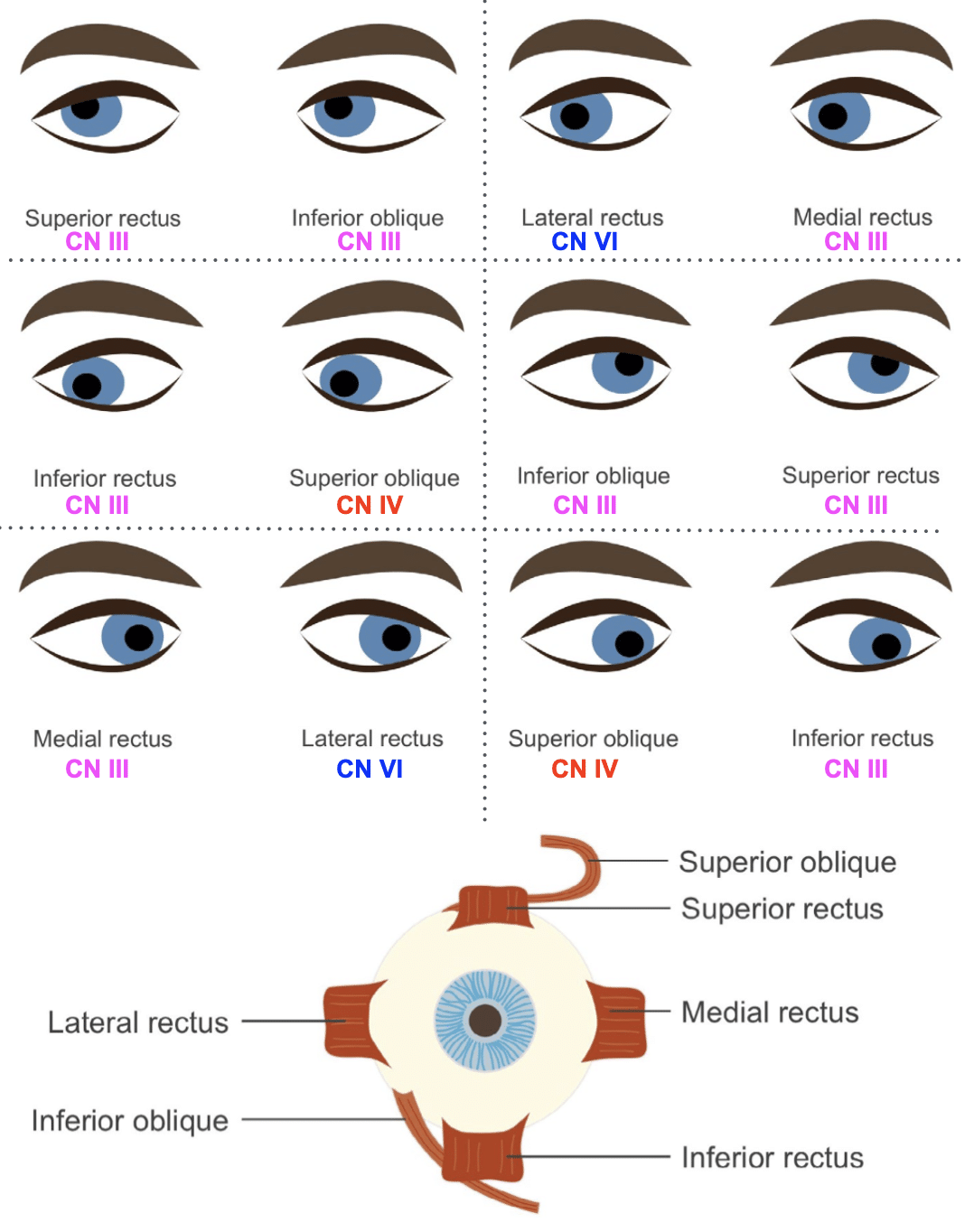
- Eye movement testing (use H pattern):
- Lateral rectus (CN VI) → horizontal outward movement
- Medial rectus (CN III) → horizontal inward movement
- When eye is abducted:
- Elevator → superior rectus (CN III)
- Depressor → inferior rectus (CN III)
- When eye is adducted:
- Elevator → inferior oblique (CN III)
- Depressor → superior oblique (CN IV)

Investigations
Blood Tests
- FBC
- CRP
- ESR
- U&Es / glucose
CT Scan / CT Angiogram
- Good screening test for intracranial mass lesions.
- CT angiogram for suspected aneurysmal disease.
MRI
- Best imaging modality.
- Detects:
- Intracranial mass lesions
- Neural lesions (e.g. MS plaques)
- May also visualise the nerve itself.
Management
- Management is directed at the cause, where established.
Appendix 1
References
Publications
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Fuller G. Neurological Examination Made Easy. 6e 2019
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
FOAMed
- Coni R. Neuro 101: Cranial Nerves. LITFL
- Nickson C. More Befuddling Pupillary Asymmetry. LITFL
- Nickson C. Third Cranial Nerve Lesions. LITFL
- Nickson C. Cranial nerve lesions DDx. LITFL
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |