
![]()
Fourth Cranial Nerve Lesions
Cranial nerve IV is also known as the Trochlear nerve.
It is a purely motor nerve and innervates only one eye muscle – the superior oblique muscle.
Isolated lesions of the trochlear nerve are very rare.
It is more commonly associated with third cranial nerve lesions.
Anatomy
Course of the Trochlear Nerve
- Originates in the trochlear nucleus, in the ventral midbrain.
- Nerves cross (decussate) around the aqueduct to the contralateral side of the brainstem prior to exiting.
- Each superior oblique muscle is supplied by fibres from the trochlear nucleus of the opposite side.
- Exits the brainstem on the dorsal surface of the midbrain, below the inferior colliculus.
- The only cranial nerve to exit the brain from its dorsal surface
- Curves around the cerebral peduncle, runs forward in the lateral wall of the cavernous sinus, between:
- Oculomotor nerve (above)
- Ophthalmic nerve (below)
- Enters the orbit via the superior orbital fissure (external to the common tendinous ring), passing:
- Below the frontal nerve
- Above the superior ramus of the oculomotor nerve
- Within the orbit, travels medially and diagonally across and above the levator palpebrae superioris and superior rectus, to innervate the superior oblique muscle.
Trochlear Nerve Innervations
| Function | Structure Innervated |
|---|---|
| Motor | Superior oblique muscle |
Pathology
Injury to the trochlear nucleus within the brainstem causes contralateral paralysis. Injury to the trochlear nerve after it exits the brainstem causes ipstilateral paralysis.2
Causes of a fourth cranial nerve lesion include:
- Demyelinating disease
- Multiple sclerosis
- Vascular disease
- Brainstem microvascular strokes
- Space-occupying lesions
- Tumours
- Aneurysms
- Abscesses
- Raised intracranial pressure
- Venoms
- Snake bite
- Thiamine deficiency
- Wernicke’s encephalopathy (as part of ophthalmoplegia)
- Trauma
- Skull base trauma
- Mononeuritis
- Diabetes
- Toxins
- Microvascular disease
- Paraneoplastic disease
- Connective tissue disease
- Infections (HIV, Lyme disease, syphilis)
- Idiopathic
- No clear cause found in some cases
- Rarely
- Cavernous sinus thrombosis
Clinical Assessment
Important Points of History
- Presenting problem usually diplopia.
- If headache present, raises suspicion for:
- Cerebral aneurysm (acute bleed or expansion)
- Intracranial tumour
- Raised intracranial pressure
Important Points of Examination
- Strabismus
- May be an obvious squint of the affected eye.
- Head tilt
- Patient may tilt head away from the lesion (towards the opposite shoulder) in an attempt to maintain binocular vision.
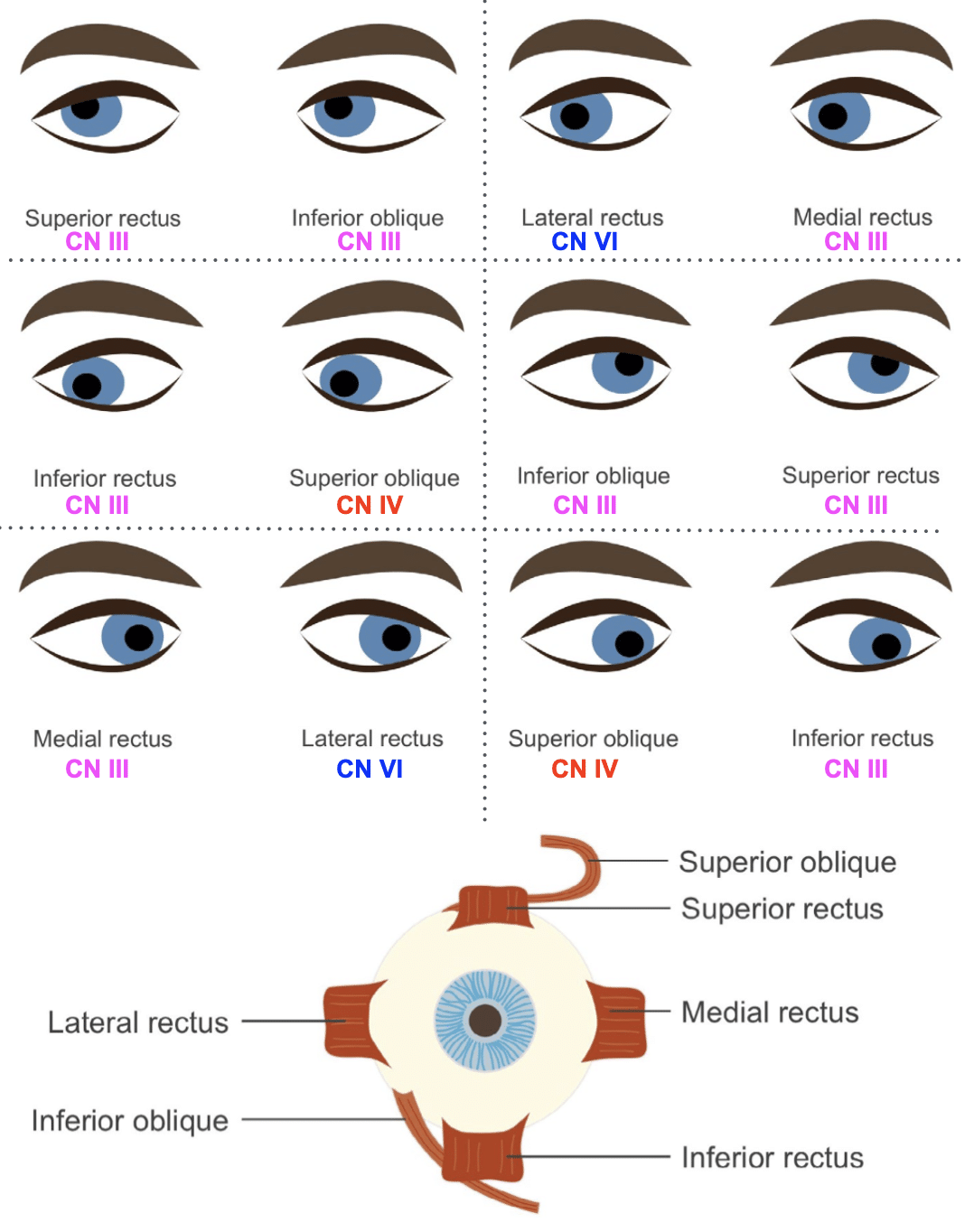
- Eye movement testing (use H pattern):
- Lateral rectus (CN VI) → horizontal outward movement
- Medial rectus (CN III) → horizontal inward movement
- When eye is abducted:
- Elevator → superior rectus (CN III)
- Depressor → inferior rectus (CN III)
- When eye is adducted:
- Elevator → inferior oblique (CN III)
- Depressor → superior oblique (CN IV)

Investigations
Blood Tests
- FBC
- CRP
- ESR
- U&Es / glucose
CT Scan / CT Angiogram
- Good screening test for intracranial mass lesions.
- CT angiogram for suspected aneurysmal disease.
MRI
- Best imaging modality.
- Detects:
- Intracranial mass lesions
- Neural lesions (e.g. MS plaques)
- May also visualise the nerve itself.
Management
- Management is directed at the cause, where established.
- Favourable prognosis if underlying cause is ischaemia (generally improves within 6 months)
- Disposition: likely Neurology ro Ophthalmology
Appendix 1
References
Publications
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Fuller G. Neurological Examination Made Easy. 6e 2019
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
FOAMed
- Coni R. Neuro 101: Cranial Nerves. LITFL
- Nickson C. More Befuddling Pupillary Asymmetry. LITFL
- Nickson C. Third Cranial Nerve Lesions. LITFL
- Nickson C. Cranial nerve lesions DDx. LITFL
Fellowship Notes

MBBS - The University of Adelaide, LMusA. Emergency Medicine registrar currently working at Sir Charles Gairdner Hospital with an interest in medical education. Classical music fanatic and pilates enthusiast.

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |