
![]()
Funtabulously Frivolous Friday Five 316
Just when you thought your brain could unwind on a Friday, you realise that it would rather be challenged with some good old fashioned medical trivia FFFF, introducing the Funtabulously Frivolous Friday Five 316
Question 1
The French call it “Rouget du porc” and the Italians call it “Mal rossino” but what does this english butcher below have:

Reveal the funtabulous answer
Well the English would call it ‘swine erysipelas’. Its original name is Baker-Rosenbach disease.
Erysipeloid is a self-limited, localized infection occurring most commonly on the finger or hand. It is caused by a rod-shaped, gram positive, faculative aerobe, E.rhusiopathiae. The bacterium may be isolated from the mucoid exterior slime covering fish, the skin and fur of animals, and both soil and water contaminated by infected animals. Because the etiologic bacterium is carried by animals it occurs most commonly in farmers; animal breeders, and veterinarians; slaughterhouse workers and butchers; fishermen (both professional and sport); chefs and others involved in food preparation; and grocery store workers who handle fresh seafood, poultry or meat. Non-occupational cases are rare.
So an occupational history is key to the diagnosis!
The lesions are well-defined, indurated, inflammatory plaque with a distinctive red-purple colour (see image above). Vesiculo-bullous and erosive areas may be present. Edema, particularly of the fingers, may be severe. The entire lesion ultimately spreads centrifugally.
Pick your favourite penicillin, cephalosporin or even clindamycin to speed up the patients recovery and prevent rare complications. The only antibiotics that don’t work are trimethoprim-sulfamethoxazole and tetracycline.
Reference:
- Dermatology advisor – Erysipeloid
- Rosenbach disease and Erysipeloid eponyms
Question 2
A 68yr old female presents with hypothermia, hypoglycaemia and a heart rate of 45 (sinus). It looks like on initial tests she has pneumonia and her sodium comes back on a VBG at 124. You think to your self, is this cold sepsis or something else, her face looks puffy and she has thinned out hair. Light bulb moment – could this be myxoedema coma? But you know your TSH/T4 won’t be back for hours.
What clinical sign can you elicit with a tendon hammer to prove your diagnosis?
Reveal the funtabulous answer
Slowness of both the contraction and the relaxation of muscles in hypothyroid patients, best seen as the “hung-up” ankle jerk and occurring because of mechanical factors and slowness of contraction time, as in myotonia and pseudomyotonia
The sign has also been demonstrated in treatment with β-blockers; diabetes mellitus; and complete heart block.
In addition to the advantages, already mentioned, of eliciting reflexes by percussion of the examiner’s finger, it should be pointed out that this method is the best available for estimating and comparing the speed of contraction and relaxation of the muscle which has been stimulated reflexly. By no other method is one as likely to recognize the presence of Woltman’s sign of myxedema. Recognition depends on observing the marked slowing of relaxation, particularly easily observed in the biceps, quadriceps, gastrocnemius, and soleus reflexes. This sign is invaluable as a clinical test for confirming the diagnosis in a case of suspected myxedema; or, as often happens in practice, the recognition of slow relaxation of reflexes may initiate the suspicion of myxedema in the first place
Bastron et al 1956: 188
- Henry Woltman (1889 – 1964)
- Chaney WC. Tendon Reflexes in Myxedema: A Valuable Aid in Diagnosis. JAMA. 1924; 82(25):2013-2016 [Woltman sign]
Question 3
This is Wunderlich’s law (1868)
Propositions relative to the temperature in typhoid fever:
- Any disease in which the temperature reaches 40°C on the evening of the first day is not a typhoid fever.
- Any illness in which the temperature does not reach 39.5°C on the evening of the fourth day is not typhoid fever.
- In typhoid fever the maximum temperature is first shown in the evening.
- On the seventh day there is a drop in temperature which never goes back to normal.
- Defervescence is always done by lysis.
- …These laws are by no means absolute.
Who was Wunderlich and why is his work relevant to us today?
Reveal the funtabulous answer
Carl Reinhold August Wunderlich (1815 – 1877) was a German physician, pioneer, and clinical academic, who is generally regarded as the father of clinical thermometry.
Clinical Thermometry (1868)
Clinical thermometry before Wunderlich’s time had sparingly been utilized and scientifically documented. It was only Hermann Boerhaave, with his students Gerard L.B. Van Swieten, Anton De Haen, and separately George Martine, who started to use the thermometer at the bedside in the 18th century. De Haen studied diurnal changes in normal subjects and observed changes in temperature with shivering or fever, and he noted the acceleration of the pulse when body temperature was elevated. De Haen found that temperature was a valuable indication of the progress of an illness. However, his contemporaries were unimpressed with the findings, and the thermometer would remain to be not widely used.
It was not until the late 19th century that clinical thermometry started to gain traction, and Wunderlich was not the only clinician interested. William Aitken, a Professor of Pathology at the British Army Medical School, had designed a newer style clinical thermometer in 1852 in an attempt to solve the issue regarding the thermometer’s large size. Thomas Clifford Alburt, a prominent English physician of the time, improved on Aitken’s design to create a portable, more efficient 6-inch clinical thermometer in 1866, and published a paper on the topic of medical thermometry in 1870.
However, no clinician was able to match the sheer volume of data Wunderlich had accumulated to write his opus, Das Verhalten der Eigenwärme in Krankheiten; the same paper in which his eponymous law is famously derived from. Utilizing the older style foot-long thermometer, which required 20 minutes to determine a patient’s temperature, Wunderlich obtained over a million axillary readings from 25,000 different patients, from which he established principles, such as diurnal temperature variation, effects of aging and sex on temperature, and the correlation of fever to illness severity, which are still taught and utilized by medicine to this day.
Future studies found that the numerical data Wunderlich presented was flawed. Indeed, Wunderlich stated in his work that the upper limit of normal temperature was 38°C (100.4°F); higher than what is commonly accepted today. Speculation exists that this may be due in part to a lack of computational technology access, the fact that statistical analysis was not commonly performed until the 1890s, and the possibility that the thermometer Wunderlich used may have been inaccurate or not properly calibrated.
Despite the inaccuracies, Wunderlich’s work carried the concept of clinical thermometry one step further than others before had done and placed it back to being a measure worthy of scientific scrutiny. Arguably, the greatest contribution to arise from the work is that fever would be recognized more appropriately as a clinical sign rather than a disease.
Question 4
Ever heard of the Sherren triangle as a sign in appendicitis? – go on, give it your best guess.
What does this sign refer to?
Reveal the funtabulous answer
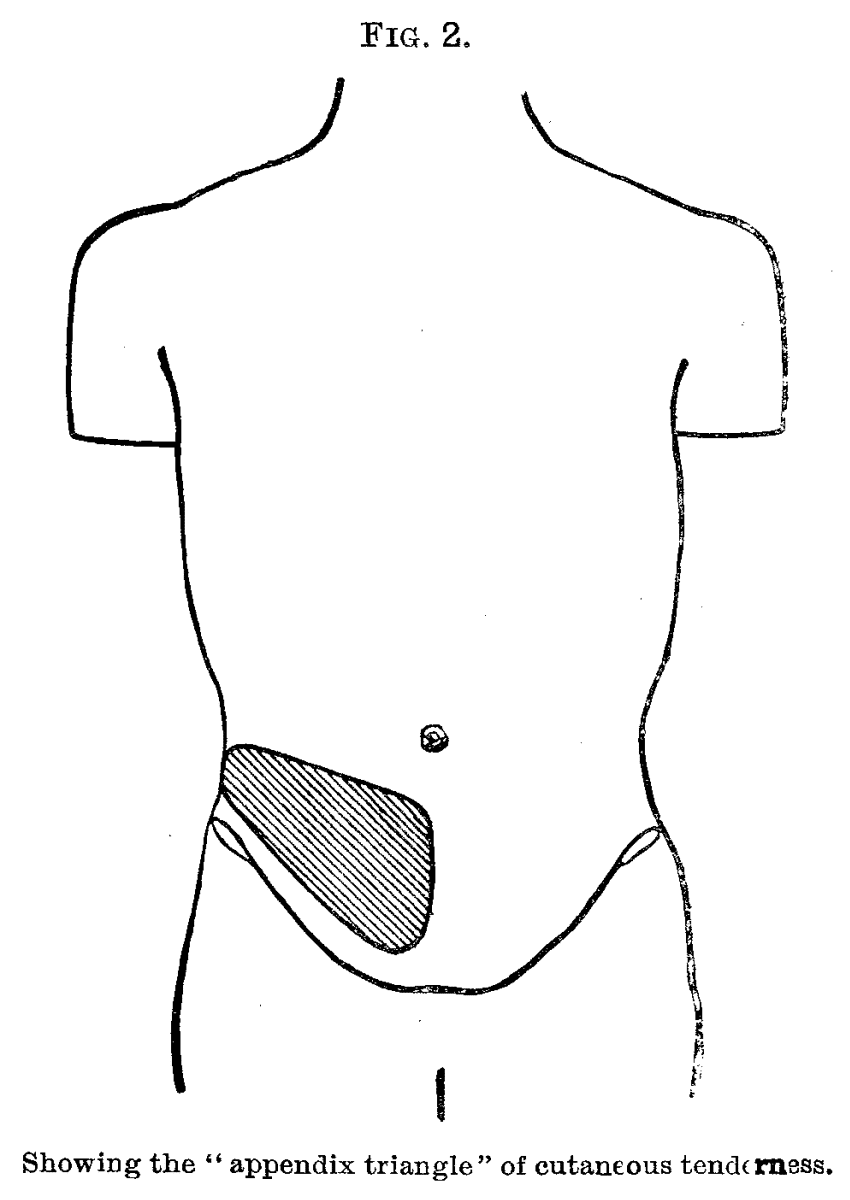
Appendix triangle of hyperaesthesia
Area of skin hyperaesthesia bounded by lines joining anterior superior iliac spine, the pubic symphysis and umbilicus which is an indication that the appendix is distended and may burst at any moment hence immediate surgery is needed.
James Sherren (1872-1945) was a British General surgeon.
- James Sherren (1872-1945) was a British General surgeon.
- Sherren J. On the occurrence and significance of cutaneous hyperalgesia in appendicitis. Lancet 1903; 162(4177): 816-821
- Eponymythology: Appendicitis eponymous signs. LITFL
Question 5
A 45yr old female presents with shortness of breath, sats of 89% and no prior medical history. No fevers and certainly no features suggestive of covid19. The following chest X-ray is thrust in your vision.
What is the diagnosis? (clue look at the right hilum)

Reveal the funtabulous answer
Pulmonary Embolism – Demonstration of Palla Sign.
Palla sign describes right descending pulmonary artery enlargement on chest x-ray, with the characteristic ‘sausage-shaped’ appearance as a potential sign of pulmonary embolism.
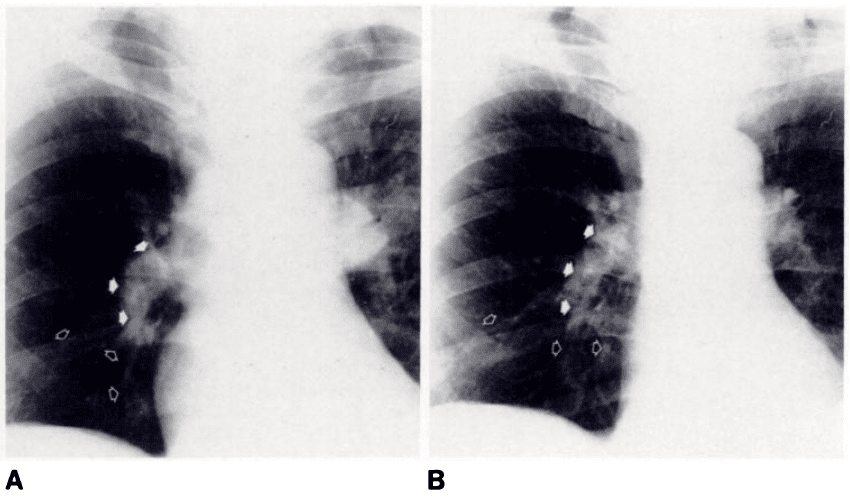
- A: CXR of patient with PE with ‘sausage’ appearance of right descending pulmonary artery (solid arrows). Lowest solid arrow points to cut-off ending; branches for middle and lower lobes are hardly visible (open arrows).
- B: 30 days later. Right descending pulmonary artery appears smaller and less dense than in previous film, with cylindrical appearance (solid arrows). Branches for middle and lower lobes appear more regular and clearly visible (open arrows).
From the practical point of view, the enlargement of descending pulmonary artery may be useful to raise the suspicion of pulmonary embolism. As documented here, the descending pulmonary artery was wider in patients with confirmed pulmonary embolism than in those without confirmation.The typical ‘sausage’ appearance of the descending pulmonary artery, easily recognizable without any measurement, was present in about one-fourth of the patients with confirmed pulmonary embolism and it was never observed in patients in whom the original clinical suspicion of pulmonary embolism was rejected subsequently.
Palla 1983
- Antonio Palla (1950 – )
- Chang CH, Davis WC. A Roentgen sign of Pulmonary Infarction. Clin Radiol. 1965; 16: 141-7.
- Palla A, Donnamaria V, Petruzzelli S, Rossi G, Riccetti G, Giuntini C. Enlargement of the right descending pulmonary artery in pulmonary embolism. AJR Am J Roentgenol. 1983; 141(3): 513-7.
- Cadogan M. CXR eponyms in pulmonary embolism. LITFL
…and finally


FFFF
Funtabulously Frivolous Friday Five
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.