
![]()
Heinrich Quincke
Heinrich Irenaeus Quincke (1842-1922) was a German physician.
Quincke is best known for several eponymous clinical signs and syndromes. His 1868 description of the capillary pulse (Quincke’s pulse) in aortic insufficiency. In 1882, he published the first detailed account of acute circumscribed oedema (Quincke’s oedema). In 1891 he introduced the lumbar puncture (Quincke’s puncture) and the Quincke spinal needle at the Congress of Internal Medicine in Wiesbaden. He also identified the fungal agent later named Trichophyton quinckeanum in 1886, and in 1871 described the triad of haemobilia: jaundice, right upper quadrant pain, and gastrointestinal bleeding known as Quincke’s triad.
He also published on poikilocytosis in pernicious anaemia, haemolysis, caisson disease, nephritic oedema, diabetic coma, and gastrointestinal therapeutics. He co-authored texts on pulmonary surgery and liver disease and served as Professor of Medicine at the universities of Bern and Kiel. Though nominated for the Nobel Prize in 1909 and again unanimously recommended in 1918, he was ultimately denied the honour.
Biographical Timeline
- Born on August 26, 1842 in Frankfurt an der Oder, Germany
- 1858–1863 – Commenced and completed medical studies at Friedrich-Wilhelm-Universität in Berlin; also studied at Würzburg and Heidelberg under Virchow, Kölliker, Müller, Helmholtz, Bunsen, and Langebeck.
- 1863 – Earned doctorate in Berlin.
- 1865 – Studied and visited hospitals in Vienna (with Ernst von Brücke), Paris, and London.
- 1866 – Appointed assistant in surgery at Bethanien Hospital, Berlin.
- 1867–1871 Assistant physician at Charité Hospital, Berlin under Friedrich Theodor von Frerichs; collaborated on cerebrospinal fluid studies in dogs.
- 1870 – Professor and director of the department of internal medicine in Bern, Switzerland
- 1871 – Reported aneurysm of the hepatic artery (Quincke’s triad).
- 1873 – Appointed Professor of Medicine, University of Bern, replacing Bernhard Naunyn (1839–1925).
- 1878 – Professor of medicine and head of internal medicine department at the University of Kiel (Christian Albrechts University), Germany; served 30 years
- 1886 – Described Trichophyton quinckeanum, causative agent of mouse favus.
- 1891 – Introduced lumbar puncture (“Quincke’s puncture”) at the Wiesbaden Congress; first cases reported in hydrocephalus and tuberculous meningitis.
- 1893 – Described idiopathic intracranial hypertension (“serous meningitis”).
- 1900 – Appointed Rector Magnificus of Kiel University
- 1903 – Co-authored Grundriss der Lungenchirurgie with Carl Garré; foundational work in lung surgery.
- 1908 – Retired from Kiel; moved to Frankfurt am Main.
- 1914–1918 Lived through WWI; wife Bertha volunteered with the Red Cross. Quincke remained active in patient care despite wartime hardship. Awarded honourary professor at Goethe University (Johann Wolfgang Goethe-Universität), Frankfurt am Main
- Died on May 19, 1922 in Frankfurt am Main. Official cause of death listed as suicide (“shot in the mouth”).
Medical Eponyms
Quincke’s pulse (1868)
An alternate paling and flushing of the skin at the root of the nail while pressure is applied to the tip of the nail, classically observed in patients with aortic regurgitation.
In 1868, at just 26 years of age, Heinrich Quincke published his observations on capillary and venous pulsations while working as an assistant at the Medical Clinic in Berlin. He described the capillary pulse as a visible, rhythmic change in nailbed coloration, best seen at the junction between the pale lunula and the pink nailbed.
As far as the capillary pulse is concerned, so can one see it best on his own finger nail, or better, on that of another, in the area between the whitish, blood-poor area and the red injected part of the capillary system of the nail-bed; in the majority of persons examined, there is, with each heartbeat, a forward and backward movement of the margin between the red and white part..
Quincke 1868
He noted that while this sign can be observed in many healthy individuals, it becomes particularly conspicuous in cases of aortic insufficiency due to the bounding, high-volume pulse:
A large and rapidly falling pulse is seen especially in aortic insufficiency, and for this reason the capillary pulse is especially clear in this condition.
Quincke 1868
Quincke’s triad (1871)
Triad of right upper quadrant pain, jaundice, and upper gastrointestinal bleeding indicative of hemobilia (bleeding into the biliary tract)
In 1871, Quincke published a detailed case of hepatic artery aneurysm rupture leading to bleeding into the biliary tree in Ein fall von Aneurysma der Leberarterie. He described the three cardinal features now recognised as Quincke’s triad.
Original
English
Die Krankheit begann…mit Kolik, Erbrechen und etwas Blutbeimengung im Stuhl… Der Kranke war bleich, hatte leichten Ikterus… gegen Abend Bluterbrechen…Wiederholte Blutungen aus dem Magen und schwarzer Stuhl wechselten mit Gelbsucht und Schmerzanfällen im rechten Hypochondrium – Quincke 1871
The illness began…with colic, vomiting and some blood in the stool…The patient was pale, had slight jaundice…in the evening he vomited blood…Repeated bleeding from the stomach and black stools alternated with jaundice and attacks of pain in the right hypochondrium – Quincke 1871
Quincke’s oedema (1882)
Also known as angioneurotic oedema or Quincke’s disease, this condition presents as sudden, transient, non-pitting oedematous swellings of the skin and subcutaneous tissues—most commonly affecting the lips, eyelids, face, extremities, and gastrointestinal mucosa.
Although Heinrich Quincke formally described the condition in 1882, earlier mentions had been made by Robert James Graves (1796-1853) in 1843 (as “fugitive inflammation”) and John Laws Milton (1820–1898) in 1876, who used the term “giant urticaria.”
I wish to identify a skin disease which does not seem to be rare; however, only a few cases of it have been described. This disease appears as oedematous swelling of the skin and the subcutaneous tissue in localized lesions from 2 to 10 cm. or more in diameter… Particularly on the lips and eyelids… Localized swellings also appear in the gastrointestinal mucosa producing symptoms… Because of its manner of development, acute localized swelling of the skin and mucous membranes, it should be considered as an angioneurosis
Quincke 1882
The lesions are often painless, without itching, and typically resolve within hours to days. In modern medicine, hereditary forms of this condition are linked to C1 esterase inhibitor deficiency and excessive bradykinin production.
Quincke’s puncture (1891)
The introduction of lumbar puncture as a diagnostic and therapeutic method for withdrawing cerebrospinal fluid (CSF) was one of Quincke’s most impactful contributions to medicine.
Quincke studied CSF physiology in dogs including the communication between the cerebral and spinal subarachnoid spaces. He hypothesized that withdrawing CSF might relieve pressure in children with hydrocephalus. He first presented the method publicly at the Congress of Internal Medicine in Wiesbaden at the Fifth sitting on Wednesday morning, April 8, 1891.
The fluid was withdrawn via a fine needle between the third and fourth lumbar vertebrae… with the help of a stylet. Pressure readings were taken before and after drainage… and samples analysed for protein, sugar, cells, and bacteria.
Quincke 1891
He performed his first lumbar puncture in 1888 on a 12-year-old boy with hydrocephalus. Unfortunately the child died despite six procedures. In 1890, he treated a 21-month-old child with suspected tuberculous meningitis who recovered after three lumbar punctures. His third case, a 25-year-old man with chronic hydrocephalus and severe headaches, improved after the procedure.
Quincke’s landmark publication, Die lumbalpunction des hydrocephalus (1891), described lumbar puncture in ten patients (five children and five adults) and detailed both technique and early diagnostic value.
In the same year, Walter Essex Wynter (1860–1945) also attempted pressure relief in paediatric meningitis, but by a surgical drainage route (incision and trocar/tube) rather than a needle puncture. Quincke’s crucial advance was that his method was minimally invasive, repeatable, and scalable. He standardised entry at the lumbar interspace, connected the needle to tubing/glass for manometry, drained CSF drop-by-drop, and recognised diagnostic possibilities (appearance, specific gravity, protein/cells/bacteria). In his September 1891 paper he even notes that his method was similar in principle to Wynter’s, while being technically simpler and more reproducible.
Although met with initial skepticism, his method became a cornerstone of neurological investigation and CSF sampling.
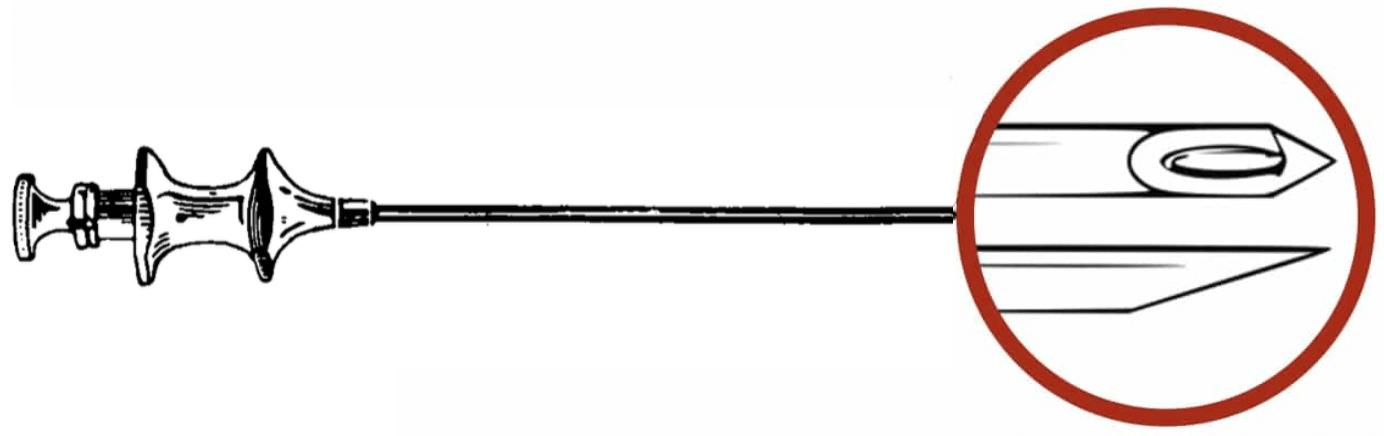
The classic Quincke spinal needle (Kanülen, nach Quincke), with its A-bevel cutting tip and Luer lock hub enabled lumbar puncture and spinal anaesthesia/
- Tip design: Sharp, cutting bevel
- Mechanism: Cuts longitudinal dural fibres, leaving a gaping dural defect
- Advantages: Reliable CSF flow, easy injection
- Disadvantages: High incidence of post–dural puncture headache (PDPH)
- Historical role: Enabled lumbar puncture and spinal anaesthesia but established the problem of PDPH
Achorion of Quincke (1886)
Quincke described the α-Pilz (“alpha fungus”) dermatophyte in 1886 as the causative agent of mouse favus. It is now taxonomically recognised as Trichophyton quinckeanum.
In Über Favuspilze (1886), Quincke reported several cases of superficial fungal infections acquired from mice, including a young girl who developed facial lesions after playing in a stable. From both human and mouse specimens, he cultivated and described the causative organism:
The α-Pilz is distinguished by its pointed spores… a species found on the skin of infected mice and transmissible to humans.
Quincke 1886
Favus caused by this organism is rare but notable for its zoonotic origin and characteristic “mousy” odour. Taxonomists reclassified Quincke’s α-Pilz as Trichophyton quinckeanum, placing it among the dermatophytes distinct from T. mentagrophytes. Cultures typically display a white, crateriform growth with reduced micromorphology and pyriform microconidia.

Recent morphological studies confirm the unique features of T. quinckeanum, including:
- Filiform appendages on macroconidia
- Absence of spiral hyphae
- Varieties adapted specifically to white or grey mice
- High CO₂ culture promoting “star-like” growth patterns and sporulation
Quincke’s discovery marked one of the earliest documented cases of direct animal-to-human mycotic transmission and remains a cornerstone in medical mycology.
Key Medical Attributions
Mallory-Weiss Syndrome (1879)
The eponymous term refers to George Kenneth Mallory and Soma Weiss and their 1929 description of postemetic lacerations at the gastroesophageal junction.
Quincke, then in Kiel, published Ulcus oesophagi ex digestione. He described three cases of oesophageal ulceration in the distal oesophagus, unrelated to carcinoma, corrosives, or trauma. Two patients died of massive haematemesis, one developed perforation into the pleura, and another had cicatricial stricture.
Quincke proposed the term “ulcus ex digestione” to describe an ulcer caused by the action of gastric juice upon the oesophageal mucosa, analogous to simple gastric ulcer. This was an early demonstration of oesophageal ulcer as a primary lesion and the first to connect it to fatal haematemesis.
Original
English
Die beschriebenen drei Fälle zeigen… dass im unteren Theil der Speiseröhre Geschwüre vorkommen… die durch die verdauende Einwirkung des Magensaftes entstanden sind… und daher mit dem sogenannten einfachen Magengeschwür auf eine Linie gestellt werden müssen – Quincke 1879
The three cases described show… that ulcers do occur in the lower part of the oesophagus… arising from the digestive action of gastric juice… and must therefore be placed on the same line as the so-called simple gastric ulcer – Quincke 1879
Scientific Contributions
Quincke conducted investigations into poikilocytosis and haemolysis of erythrocytes, contributing early insights into the haematologic abnormalities of pernicious anaemia and the mechanisms of haemosiderosis. His experimental work on caisson disease offered some of the first physiological explanations for decompression sickness.
In internal medicine, Quincke studied the extrarenal mechanisms of nephritic oedema, emphasizing vascular permeability rather than purely renal causes, well ahead of its time. He investigated the role of iron salts in therapy, advanced understanding of gastrointestinal nutrition in illness, and described diabetic coma.
Quincke also published on infectious diseases, including amoebic dysentery, typhoid fever, and the utility of lumbar puncture in the diagnosis of tuberculous meningitis.
Controversies
Not…The Nobel Prize
Quincke was nominated for the 1909 Nobel Prize in Physiology or Medicine for his pioneering work on lumbar puncture (first presented in 1891). However, the committee rejected the nomination, citing the 18-year delay between discovery and recognition.
In 1918, circumstances changed. A prior critic now praised Quincke’s work as being of “extraordinarily high diagnostic value.” The Nobel Committee unanimously recommended Quincke for the prize. Yet, at 76 years of age, he was ultimately passed over again, deemed too old to receive the honour.
This decision would later echo in the case of Joseph Babinski (1857–1932), and Bernhard Naunyn (1839-1925) both falling foul of ageism.
Notably, Nobel rules evolved: in 1966, Peyton Rous (1879–1970) received the Nobel Prize at age 87, for a discovery published 55 years earlier, correcting the ageist principle that once excluded Quincke, Babinski and Naunyn.
Major Publications
- Quincke H. Beobachtungen uber capillar- und venenpuls [Observations on capillary and venous pulsations]. Berliner Klinische Wochenschrift 1868; 5: 357–359. [Quincke’s pulse]
- Quincke H. Ein fall von Aneurysma der Leberarterie [A case of aneurysm of the hepatic artery]. Berliner Klinische Wochenschrift 1871; 8: 349-352 [Quincke triad]
- Quincke H. Ueber Vagusreizubg beim Menschen [Vagus stimulation in man]. Berliner Klinische Wochenschrift 1875; 12: 189-191
- Quincke H. Ulcus oesophagi ex digestione. Deutsches Archiv für klinische Medicin. 1879; 24: 72-79. [Mallory-Weiss syndrome]
- Quincke H. Über akutes umschriebenes Hautödem. [Acute circumscribed edema of the skin]. Monatshefte für praktische Dermatologie 1882; 1: 129-131 [Quincke’s oedema]
- Quincke H. Ueber Favuspilze. Archiv für experimentelle Pathologie und Pharmakologie. 1886; 22(1-2): 62–76
- Quincke HI. Ueber hydrocephalus. Verhandlungen des Congresses für Innere Medicin, Zehnter Congress, Gehalten zu Wiesbaden, vom 6.-9. April 1891: 321-339.
- Quincke HI. Die lumbalpunction des hydrocephalus. Berliner Klinische Wochenschrift 1891; 28: 929-933 and 965-968
References
Biography
- Pagel J. Heinrich Irenaeus Quincke. Biographisches Lexikon, hervorragender Ärzte des neunzehnten Jahrhunderts. 1901.
- Editorial. Heinrich lrenaeus Quincke (1842-1922) – clinician of Kiel. JAMA 1966; 196: 1152-3
- Minagar A, Lowis GW. Dr Heinrich Irenaeus Quincke (1842-1922): clinical neurologist of Kiel. J Med Biogr. 2001 Feb;9(1):12-5.
- Göring HD. Heinrich Irenäus Quincke Aus Anlass seines 160. Geburtstages und 80. Todestages sowie seiner Beschreibung des Angioödems vor 120 Jahren [In memory of the 160(th) birthday and the 80(th) anniversary of the death of Heinrich Irenäus Quincke, as well as of his description of angioedema 120 years ago]. Hautarzt. 2002 Dec;53(12):822-5
- Cozanitis DA. Heinrich Irenaeus Quincke (1842-1922): the Nobel Prize but for the problem of age. Presse Med. 2013; 42 (4.1): 464-70.
- Suwa B. Heinrich Quincke (1842–1922) and the social hygiene movement. Allergo J Int 2025; 34: 15–20
Lumbar puncture
- Frederiks JA, Koehler PJ. The first lumbar puncture. J Hist Neurosci. 1997 Aug;6(2):147-53
- Pearce J. Fragments of Neurological History Edition. Imperial College Press. 2003;203.
- Harms R, Cadogan M. History of Spinal Needles. LITFL
- Harms R, Cadogan M. History of Neuraxial Anaesthesia. LITFL
Eponymous terms
- Quincke H. Observations on Capillary and Venous Pulse. In: Major RH. Classic Descriptions of Disease, Springfield. 1945: 361-363.
- Balabanoff VA, Kasărov LB. On the morphology of trichophyton quinckeanum. Mycopathologia et Mycologia Applicata, 1963; 21(2): 119-128.
- Zhang G. Eponyms in Aortic Regurgitation. LITFL 2019
Angioneutortic oedema
- Graves RJ. Fugitive inflammation. In Clinical lectures on the practice of medicine. 1848; 1: 462-463
- Milton JL. On giant urticaria. Edinburgh medical journal, 1876; 22: 513-526
- Quincke H. Über akutes umschriebenes Hautödem. [Acute circumscribed edema of the skin]. Monatshefte für praktische Dermatologie 1882; 1: 129-131
- Bannister HM. Acute angioneurotic oedema. Journal of nervous and mental disease, 1894; 19: 627-631
Quincke Triad
- Harlaftis NN, Akin JT. Hemobilia from ruptured hepatic artery aneurysm. Report of a case and review of the literature. Am J Surg. 1977 Feb;133(2):229-32.
- Curran FT, Taylor SA. Hepatic artery aneurysm. Postgrad Med J. 1986 Oct;62(732):957-9.
- Belfonte, Cassius MB, BS; Sanderson, Andrew MD, FACG; Dejenie, Freaw MD. Quincke’s Triad: A Rare Complication of a Common Outpatient Procedure. American Journal of Gastroenterology 106():p S277, October 2011
- Jamtani I, Nugroho A, Irfan W, Fadli M, Saunar RY, Widarso A, Poniman T. Revisiting Quincke’s Triad: A Case of Idiopathic Hepatic Artery Aneurysm Presenting with Obstructive Jaundice. Ann Vasc Surg. 2021 Feb;71:536.e1-536.e4.
- Patil NS, Kumar AH, Pamecha V, Gattu T, Falari S, Sinha PK, Mohapatra N. Cystic artery pseudoaneurysm-a rare complication of acute cholecystitis: review of literature. Surg Endosc. 2022 Feb;36(2):871-880.
- Schütz ŠO, Rousek M, Pudil J, Záruba P, Malík J, Pohnán R. Delayed Post-Traumatic Hemobilia in a Patient With Blunt Abdominal Trauma: A Case Report and Review of the Literature. Mil Med. 2023 Nov 3;188(11-12):3692-3695.
- Ahmed M, Saeed R, Woodward C, Nguyen K, Auda D. Quincke’s Triad and Cystic Artery Pseudoaneurysm. Cureus. 2025 Jan 18;17(1):e77627.
Eponym
the person behind the name
Doctor in Australia. Keen interest in internal medicine, medical education, and medical history.
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |