
![]()
Henry Pancoast

Henry Khunrath Pancoast (1875-1939) was an American radiologist.
Pancoast was the First Professor of Radiology in America. The Pancoast tumour and Pancoast Syndrome are named after him.
Major work on studying the healthy chest; interpretation of silicosis, tuberculosis and pneumoconiosis X-ray; bismuth shadow interrogation of the intracranial lesions; radiotherapeutic intervention
Biography
- Born on February 26, 1875 in Philadelphia, USA (father Dr Seth Pancoast)
- 1892 – Graduated Friend’s Central School, Pennsylvania. Delayed plans to enter medical school due to the premature death of both his parents. Became a bank teller for 2 years and started Medical School in 1894 with no undergraduate premedical preparation
- 1898 – Graduated medical school from the University of Pennsylvania
- 1900 – Commenced surgical training Hospital of the University of Pennsylvania
- 1903 – Asked to join the Hospital ‘Roentgen Ray Department’ as a sciagrapher. He later remarked: “How easy it was in those days to become a radiologist by the shortest affirmative reply!“
- 1911 – First Professor of Roentgenology (Radiology) in the United States
- 1915 – Use of radium to treat inoperable carcinoma, brain tumors, uterine hemorrhage, warts, and moles
- Died on May 20, 1939
Medical Eponyms
Pancoast Tumour
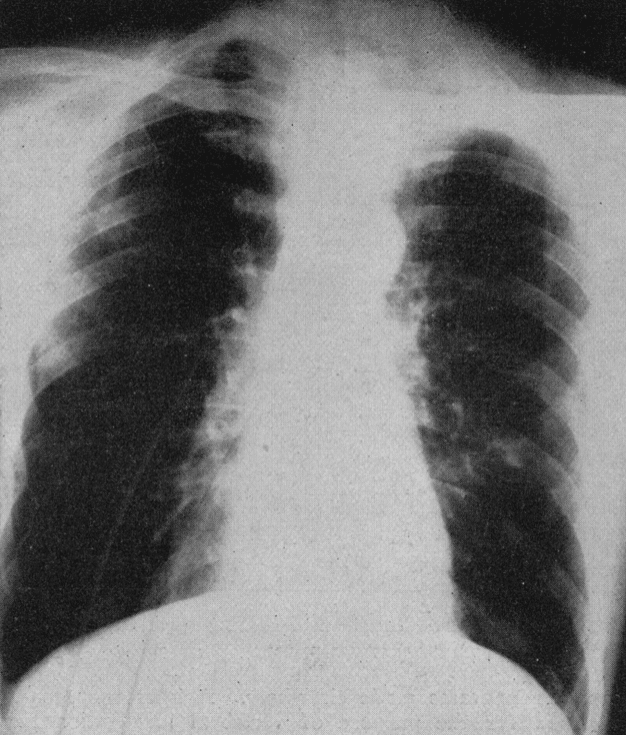
Pancoast Tumour is a primary bronchogenic carcinoma which arises in the apex of the lung at the superior pulmonary sulcus. They are usually non-small cell lung cancer (NSCLC) and interchangeably referred to as Pancoast Tumours.
1924 – Pancoast described three cases of localised apical lung tumors with neurological findings
Case 1: A man, aged 52, was admitted to the University Hospital early in September, 1921. His chief complaint was intense burning pain, high in the left axilla and extending down the arm, worse at night and keeping him awake. It was then of eleven months’ duration, at first intermittent and later continuous; limited to the shoulder girdle at first, but later referred down the arm to the elbow, and for the last two months to the wrist, during which time there was an associated muscular twitching, increasing weakness of the grip and muscular wasting of the hand.
On admission, there was noted a contracted left pupil, enophthalmos and narrowing of the palpebral fissure.
Pancoast 1924
1932 – Pancoast described 7 cases (three previous and 4 new cases). He discarded the term ‘apical chest tumor’ in favour of ‘superior pulmonary sulcus tumor‘, and incorrectly proposed the tumors as arsing from epitheleal rests of the 5th brachial cleft. “It occurred to me that this tumor as a distinct entity might take its origin in an embryonal epithelial rest.“
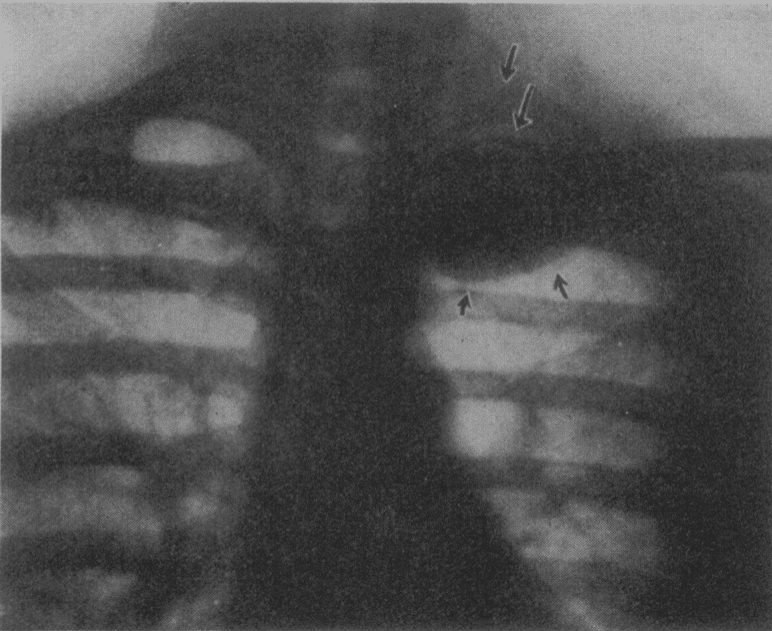
Fig. 3 (case 7).—Roentgenogram of the chest, showing the circumscribed apical shadow. Note the upper arrows pointing to the second rib and to the head and neck of the first rib, both of which are intact. Pancoast 1932
Pancoast syndrome
Pancoast Syndrome occurs secondary to local compression of brachial plexus and sympathetic chain by superior (pulmonary) sulcus tumors. Syndrome consists of:
- Shoulder pain: initially localised to shoulder and vertebral border of scapula)
- Radicular pain C8-T2: Progressive ulna nerve distribution pain and muscular atrophy
- Horner syndrome: present in 25% of presentations of Superior sulcus tumors. Extension of neoplastic invasion/compression to involve sympathetic chain and stellate ganglion
Major Publications
- Pancoast HK. Malignant disease of the throat and sinuses : review of cases treated by radium and roentgen rays. 1917
- Pancoast HK. Practical uses of the X-ray. 1917
- Pancoast HK. Importance of careful roentgen-ray investigation of apical chest tumors. Journal of the American Medical Association, Chicago, 1924; 83: 1407 [Pancoast tumour]
- Pancoast HK. Some observations on the radiation treatment of carcinoma of the larynx. 1924
- Pancoast HK, Pendergrass EP. Pneumoconiosis (silicosis) a Roentgenological study, with notes on pathology. 1926
- Pancoast HK. Superior pulmonary sulcus tumor. Tumor characterised by pain, Horner’s syndrome, destruction of bone and atrophy of hand muscles. Journal of the American Medical Association, 1932: 99: 1391-1396 [Pancoast syndrome]
- Pancoast HK, Schaeffer JP, Pendergrass EP. The Head and Neck in Roentgen Diagnosis. Thomas 1940
Controversies
Pancoast was not the first to describe the neoplasm or the associated syndrome associated with local invasion
- British surgeon Edward Selleck Hare (1812-1838) first described in 1838.
- Publio Ciuffini described lung apical tumor with local invasion in 1911.
- Pancoast described three cases in 1924 and in 1932 described the tumor as a “superior pulmonary sulcus tumor”. Pancoast incorrectly described the tumors as ‘arsing from epitheleal rests of the 5th brachial cleft’.
- J. W. Tobías correctly surmised the tumor site of origin as bronchopulmonary tissue in his 1932 publication
References
Biography
- The Pancoast Era – University of Pennsylvania
- Bibliography. Pancoast, Henry K. (Henry Khunrath) 1875-1939. WorldCat Identities
Eponymous terms
- Arcasoy, SM. Jett, JR. Superior Pulmonary Sulcus Tumors and Pancoast’s Syndrome N Engl J Med 1997; 337: 1370-1376 [Full Text] [PMID 9358132]
Our Pancoast thinks everyone crazy
Who works without skiagrams hazy,
In fact you would laugh
To hear the whole staff
Rave on as if they were X-rasy
University of Pennsylvania, Scope Yearbook – 1912
[cite]
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |