![]()
Pancoast Tumour
Description
Pancoast Tumour is a primary bronchogenic carcinoma which arises in the apex of the lung at the superior pulmonary sulcus.
Pancoast tumours most commonly demonstrate histology of non-small cell lung cancer (NSCLC) – historically usually squamous cell carcinoma, but now more commonly adenocarcinoma. Pancoast tumours account for 3-5% of all bronchogenic carcinomas. The neoplasm invades the surrounding soft tissues and 25% of tumours present with Pancoast syndrome
Typically treated with radiotherapy to downstage the tumor followed by local resection (complicated by proximity of brachial plexus and subclavian vessels). 5 year survival rate varies from 45% with complete resection to 0% with incomplete resection
Example Cases: CXR Case 064 – CXR Case 069 – Befuddler 025
History of Pancoast Tumour
Pancoast was not the first to describe the neoplasm or the associated syndrome associated with local invasion.
1838 – British surgeon Edward Selleck Hare (1812-1838) described the case of a man who had died of a tumour on his neck. He had for some time before death exhibited marked constriction of the left pupil and drooping of the Levator palpebrae sutperioris. The clinical case author Hare, died on September 28, 1838, a day before the communication was published. So far as is known, he was the first clinical observer who recorded the existence of what is now termed “Horner syndrome” in association with a cervical lesion.
1912 – Publio Ciuffini, published a case of primary cancer of the apex of the right lung. He drew the clinicians’ attention to a complex of symptoms which he believed to be characteristic. Symptoms consisted of paresis, paraesthesia, and pain in the ipsilateral arm due to compression of the brachial plexus; ipsilateral ptosis, enophthalmos and miosis; and finally compression of the subclavian artery and vein.
Original
English
Imponenti furono anche in questo paziente i fenomeni di compressione , esercitati sugli organi vicini: primo a risentire gli effetti di essa fu il plesso brachiale dello stesso lato, a cui seguì, dopo molto tempo, la paralisi unilaterale del ricorrente, la quale in seguito divenne bilaterale, rendendo completamente afono il malato. Ad essa si unirono, un mese prima della fine, gli effetti della lesione della 8th radice cervicale e della l” dorsale, la quale ebbe la sua espressione in quel ristringimento della rima palpebrale destra, in quel l’enoftalmo, nella miosi della pupilla, nella mancanza del riflesso al dolore.
Ciuffini P. Sul cancro primitivo del polmone. 1912
The compression phenomena exerted on nearby organs was impressive in this patient: the first to show the effects was the brachial plexus of the same side, followed, after a long time, by the unilateral paralysis of the recurrent laryngeal nerve, which later became bilateral, making the patient completely mute. It was joined, a month before the end, by the effects of the lesion of the 8th cervical root and of the 1st dorsal, clinically manifest with right eye ptosis, enophthalmos, miosis, and lack of pain reflex.
Ciuffini P. Sul cancro primitivo del polmone. 1912
1924 – Henry Khunrath Pancoast (1875-1939) described three cases of localised apical lung tumors with neurological findings
Case 1: A man, aged 52, was admitted to the University Hospital early in September, 1921. His chief complaint was intense burning pain, high in the left axilla and extending down the arm, worse at night and keeping him awake. It was then of eleven months’ duration, at first intermittent and later continuous; limited to the shoulder girdle at first, but later referred down the arm to the elbow, and for the last two months to the wrist, during which time there was an associated muscular twitching, increasing weakness of the grip and muscular wasting of the hand.
On admission, there was noted a contracted left pupil, enophthalmos and narrowing of the palpebral fissure.
Pancoast 1924
1932 – Pancoast described 7 cases (three previous and 4 new cases). He discarded the term ‘apical chest tumor’ in favour of ‘superior pulmonary sulcus tumor‘, and incorrectly proposed the tumors as arsing from epitheleal rests of the 5th brachial cleft. “It occurred to me that this tumor as a distinct entity might take its origin in an embryonal epithelial rest.“
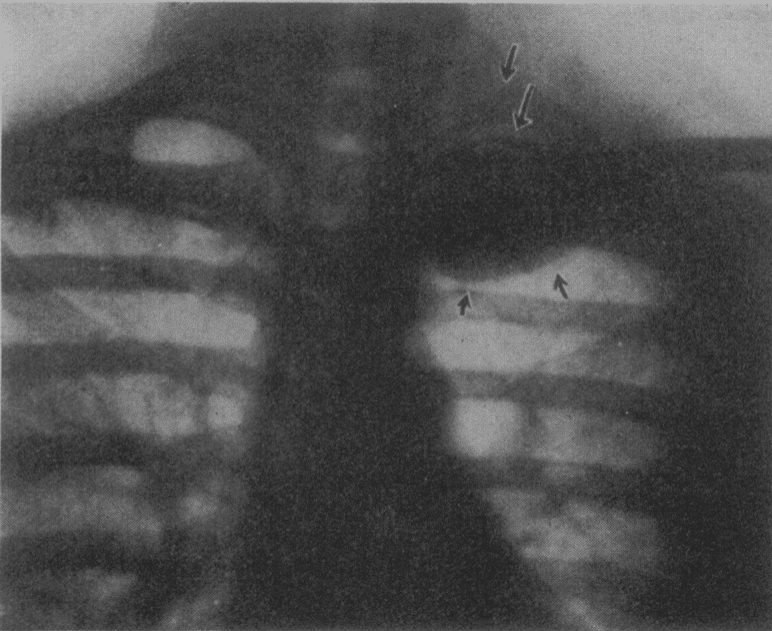
Fig. 3 (case 7).—Roentgenogram of the chest, showing the circumscribed apical shadow. Note the upper arrows pointing to the second rib and to the head and neck of the first rib, both of which are intact. Pancoast 1932
1932 – J. W. Tobías correctly surmised the tumor site of origin as bronchopulmonary tissue
Associated Persons
- Edward Selleck Hare (1812-1838)
- Publio Ciuffini
- Henry Khunrath Pancoast (1875-1939)
- José W. Tobías (1893-1951)
Alternative names
- Superior Sulcus Tumour; Pulmonary Sulcus Tumor
- Pancoast’s Tumour; Pancoast’s disease
- Hare syndrome; Tobías syndrome
- Ciuffini-Pancoast-Tobías syndrome; Ciuffini-Pancoast syndrome
References
Original articles
- Hare ES. Tumor involving certain nerves. London Medical Gazette, 2nd series, 1838/39; 1: 16-18.
- Ciuffini P. Sul cancro primitivo del polmone. Il Policlinico. Sezione medica. 1912; 19: 67-85
- Freeman W. Endothelioma of the Pleura Simulating Spinal Cord Tumor. International Clinics 1921; 31(4): 159-166
- Pancoast HK. Importance of careful roentgen-ray investigation of apical chest tumors. Journal of the American Medical Association, Chicago, 1924, 83: 1407.
- Pancoast HK. Superior pulmonary sulcus tumor. Tumor characterised by pain, Horner’s syndrome, destruction of bone and atrophy of hand muscles. Journal of the American Medical Association,1932, 99: 1391-1396
- Tobías JW. Sindrome ápico-costo-vertebral doloroso por tumor apexiano. Su valor diagnóstico en el cáncer primitivo pulmonare. Revista medica Latino-americana, Buenos Aires, 1932; 17: 1522-1557.
Review articles
- Fulton JF. Edward Selleck Hare (1812-1838) and the Syndrome of Paralysis of the Cervical Sympathetic. Proc R Soc Med. 1929 Dec;23(2):152-7.
- Baisi F. Sindrome di Ciuffini-Pancoast da cisti di echinococco dell’apertura superiore del torace [Ciuffini-Pancoast syndrome caused by echninococcal cyst of the superior thoracic cavity]. Archivio Chir Torace. 1956 Jul-Sep;13(3):399-410
- Massenti S, Racugno V. Sindrome di Ciuffini-Pancoast da cisti da echinococco apicale extrapleurica [Ciuffini-Pancoast syndrome caused by extrapleural apical echinococcic cyst]. Radiol Med. 1957 Jan;43(1):63-73.
- Mazzoni G, Di Pietro D. La sindrome di Ciuffini-Pancoast-Tobias da cisti d’echinococco [Ciuffini-Pancoast-Tobias syndrome induced by echinococcus cyst]. Policlinico Chir. 1957 Sep-Oct;64(5):299-307.
- Arcasoy, SM. Jett, JR. Superior Pulmonary Sulcus Tumors and Pancoast’s Syndrome N Engl J Med 1997; 337:1370-1376
- Weerakkody, Y. Pancoast tumour. Radiopaedia
eponymictionary
the names behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |