
![]()
Lauge-Hansen classification of ankle injury
The Lauge–Hansen classification of ankle injury describes rotational ankle fracture patterns based on a proposed sequence of injury to the syndesmosis, malleoli, and collateral ligaments. Appreciation of ankle injury mechanism furthers understanding of likely associated ligamentous injury, implications of joint stability and management.
In modern practice Lauge-Hansen is used mainly as a pattern-recognition framework (radiograph → likely mechanism → predictable associated injuries)
The Lauge-Hansen classification describes four common injury patterns each progressing through stages of ligament disruption and fracture. Three radiographic views (AP, mortise, lateral) are required and a two-word descriptor assigned:
- 1st word: foot position at injury (supination or pronation)
- 2nd word: deforming force (external rotation, adduction, abduction)
Supination Adduction (SAD) [often ~ Weber A]
- Stage 1: stress on lateral collateral ligaments results in lateral ligament rupture or lateral malleolus avulsion fracture (below level of syndesmosis).
- Stage 2: oblique fracture of medial malleolus
Supination External Rotation (SER) [often ~ Weber B] most common injury mechanism
- Stage 1: anterior syndesmosis rupture, AITFL tear
- Stage 2: oblique fracture of lateral malleolus (at level of syndesmosis)
- Stage 3: posterior syndesmosis rupture, posterior malleolus fracture, or PITFL tear
- Stage 4: medial malleolus fracture or tear of medial collateral ligaments (deltoid ligament)
Pronation External Rotation (PER) [often ~ Weber C]
- Stage 1: medial malleolus fracture or tear of medial collateral ligaments (deltoid ligament)
- Stage 2: anterior syndesmosis rupture, AITFL tear
- Stage 3: high fibula fracture (above level of syndesmosis)
- Stage 4: posterior syndesmosis rupture, posterior malleolus fracture, or PITFL tear
Pronation Abduction (PAB)
- Stage 1: medial malleolus fracture or tear of medial collateral ligaments (deltoid ligament)
- Stage 2: anterior syndesmosis rupture, AITFL tear
- Stage 3: comminuted/transverse fibula fracture (above level of syndesmosis)
The Lauge–Hansen classification assists in predicting associated ligament injury and guides further imaging options. Once a stage feature is recognised, look for the next predictable injury in the sequence. This system can be mapped conceptually to Weber/AO terminology, but the classifications are not interchangeable.
Limitations: Some fractures do not conform to the model, reproducibility is variable, and the true foot position at injury is often uncertain. Lauge–Hansen is most useful as a practical checklist rather than gospel.
Simplified diagnostic algorithm
2012 – Okanobo et al publish a simplified diagnostic algorithm and teaching approach expanding on work by Arimoto and Forrester (1980). Classify from radiographs by working logically through fibular fracture level/orientation and associated medial/posterior findings. Emphasises that stages are cumulative and radiographs can be translated back into a mechanism.
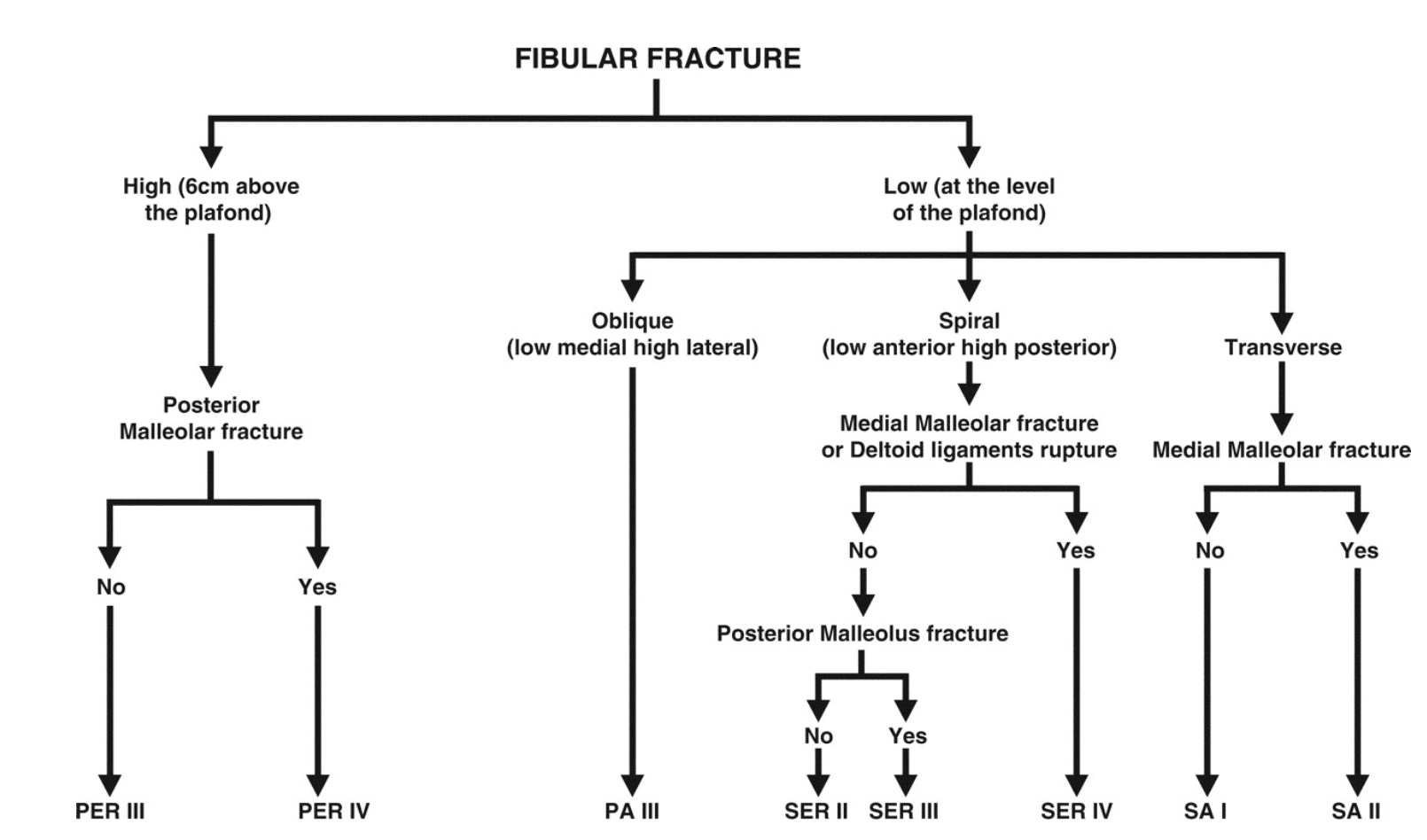
PA: Pronation Abduction, PER: Pronation External Rotation,
SA: Supination Adduction, SER: Supination External Rotation.
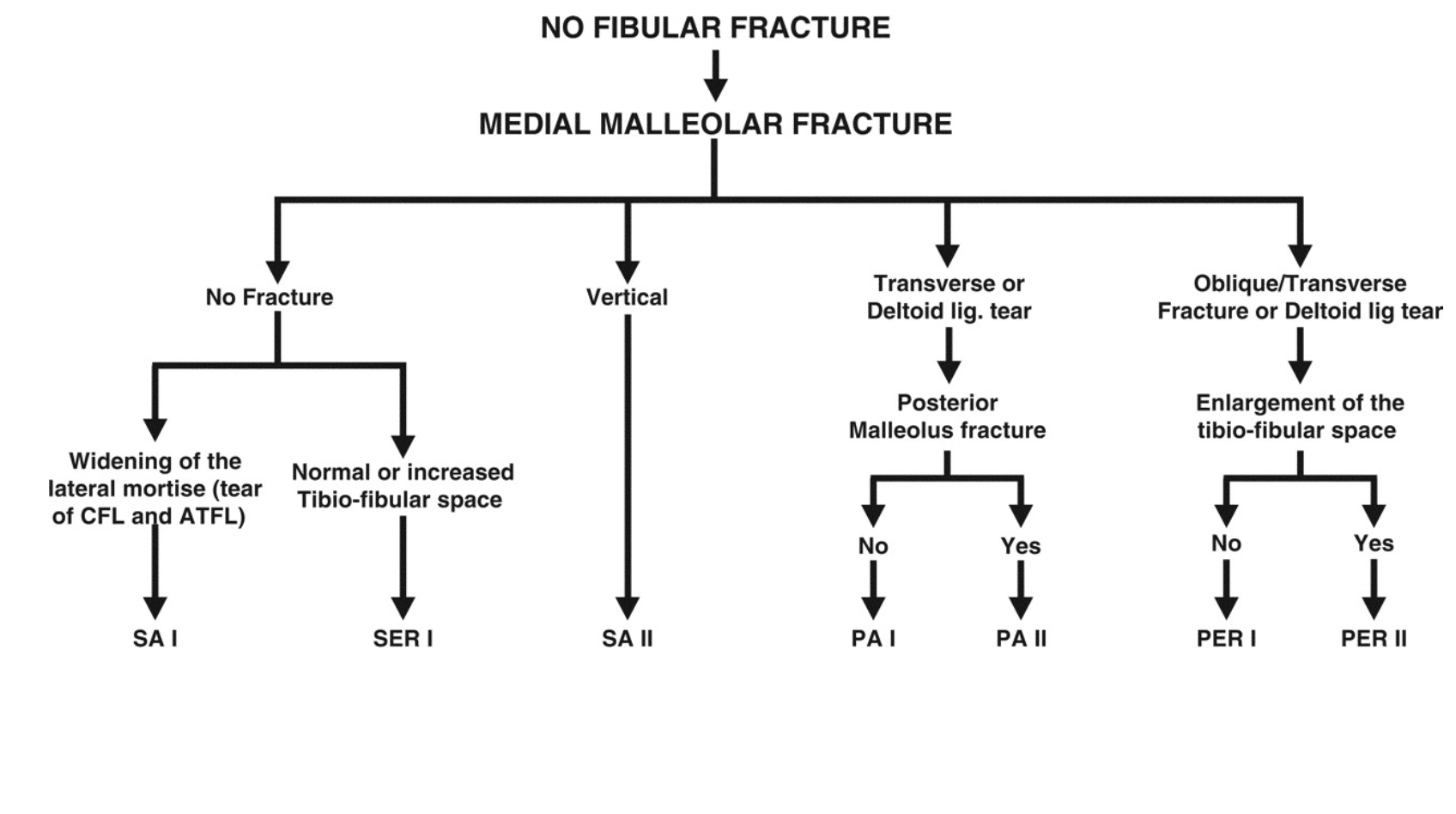
CFL: Calcaneofibular ligament, PA: Pronation Abduction, PER: Pronation External Rotation,
SA: Supination Adduction, SER: Supination External Rotation.
History of the Lauge-Hansen classification
1768 – Sir Percivall Pott (1714-1788) published Some few general remarks on fractures and dislocations, effectively the first classification system for ankle fractures. He describes fractures in terms of the number of malleoli involved, thus dividing injuries into unimalleolar, bimalleolar and trimalleolar. Easy to use, with good intraobserver reliability, it does not distinguish between stable and unstable injuries
1948 – Niels Lauge-Hansen (1899-1976) publishes an “analytic historic survey” of ankle fractures as groundwork for later experimental and clinical work.
1948 – Lauge-Hansen published his first definitive review on ankle fractures and an analytical review on the history of ankle fractures used as the basis of his future experimental, roentgenologic and clinical investigation
1949 – Robert Danis published ‘Théorie et pratique de l’ostéosynthèse‘ including discussion of malleolar fractures providing early basis to classification
1950 – In ‘Fractures of the ankle II‘, Lauge-Hansen combined experiment surgical and roentgenologic investigations to provide the earliest description of his classification. He defined ankle fractures by (1) foot position and (2) deforming force, with injuries occurring in a predictable sequence
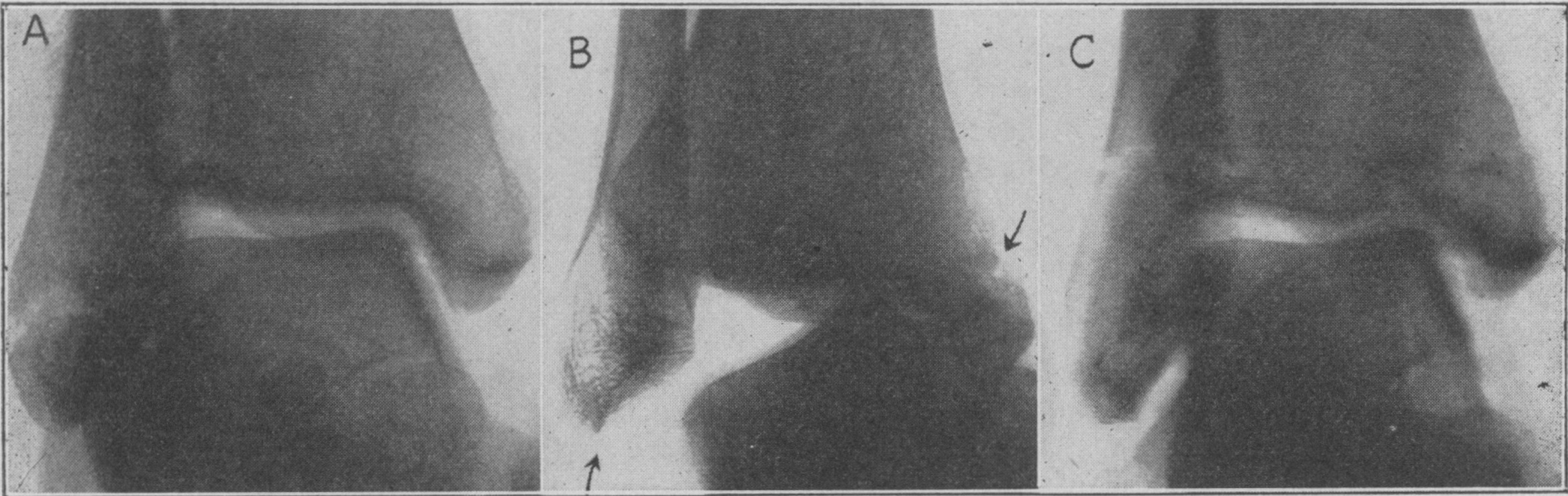
B, Supination-ADduction fracture, stage 2: detachment of the collateral lateral ligaments and fracture in the basis of the medial malleolus
C, Supination-ADduction fracture, stage 2: transverse fracture just proximal to the lateral malleolus (clinically a rare form of the fracture) and fracture in the basis of the medial malleolus. Lauge-Hansen 1950
1952-1954 – Lauge-Hansen published ‘Fractures of the ankle IV: Clinical use of genetic roentgen diagnosis and genetic reduction’ (1952); ‘Fractures of the ankle V: Pronation-dorsiflexion fracture’ (1953) and ‘Fractures of the ankle III: Genetic roentgenologic diagnosis of fractures of the ankle’ (1954)
1972 – Bernhard Georg Weber developed and popularised the Danis-Weber classification system widely used due to simplicity and reproducibility.
Reliability and biomechanical critique
1990 – Reproducibility concerns formalised: assessment of Lauge–Hansen reproducibility in clinical radiographs (118 cases) demonstrates limited agreement across observers.
1997 – Modern biomechanical attempts struggle to reproduce classic SER patterns using Lauge-Hansen’s proposed cadaver method (example cited in reviews).
2006 – MRI-based work questions whetrately predicts associated ligament injury in practice (radiograph vs MRI discordance).
“Real-world mechanism” validation attempts
2010/2013 – Kwon et al and Rodriguez et al studied YouTube videos and correlated mechanisms of injury with radiographic findings. They found that when injury video clips were matched to their corresponding X-rays, the Lauge-Hansen classification system had a 65% (17 of 26 ankle fractures) consistency rate in predicting fracture patterns from the deforming-injury mechanism. However the AO/OTA classification system had an improved consistency rate of 81% (21 of 26 ankle fractures)
Modern-day interpretation (CT/MRI and outcomes)
2015: Major “state of play” reviews emphasise: fair-at-best interobserver reliability, difficulty assigning true mechanism, and the need to combine systems; also highlight fractures that don’t fit the schema (e.g., isolated posterior margin patterns).
2025: Contemporary research still uses Lauge–Hansen categories as clinically meaningful groupings:
- Rotational fracture outcomes (SER vs PER, grade III/IV) after ORIF—similar functional/radiographic outcomes but longer fibular union time in PER.
- MRI T2 mapping of talar cartilage analysed by Lauge–Hansen mechanism groupings (supination vs pronation, posterior malleolus involvement), reflecting an ongoing shift toward mechanism-linked cartilage/soft-tissue phenotyping
Associated Persons
- Sir Percivall Pott (1714-1788) [Pott fracture]
- Niels Lauge-Hansen (1899-1976) [Lauge-Hansen classification]
- Robert Danis (1880-1962) [Danis-Weber classification]
- Bernhard Georg Weber (1927-2002) [Weber classification]
References
Original articles
- Lauge-Hansen N. Ligamentous ankle fractures; diagnosis and treatment. Acta Chir Scand. 1949 Mar 23;97(6):544-50.
- Lauge-Hansen N. Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Arch Surg. 1950 May;60(5):957-85.
- Lauge-Hansen N. Fractures of the ankle. III. Genetic roentgenologic diagnosis of fractures of the ankle. Am J Roentgenol Radium Ther Nucl Med. 1954 Mar;71(3):456-71.
- Lauge-Hansen N. Fractures of the ankle. IV. Clinical use of genetic roentgen diagnosis and genetic reduction. AMA Arch Surg. 1952 Apr;64(4):488-500.
- Lauge-Hansen N. Fractures of the ankle. V. Pronation-dorsiflexion fracture. AMA Arch Surg. 1953 Dec;67(6):813-20.
Review articles
- Arimoto HK, Forrester DM. Classification of ankle fractures: an algorithm. AJR Am J Roentgenol. 1980 Nov;135(5):1057-63.
- Okanobo H, Khurana B, Sheehan S, Duran-Mendicuti A, Arianjam A, Ledbetter S. Simplified diagnostic algorithm for Lauge-Hansen classification of ankle injuries. Radiographics. 2012 Mar-Apr;32(2):E71-84.
- Gardner MJ, Demetrakopoulos D, Briggs SM, Helfet DL, Lorich DG. The ability of the Lauge-Hansen classification to predict ligament injury and mechanism in ankle fractures: an MRI study. J Orthop Trauma. 2006 Apr;20(4):267-72.
- Kwon JY, Chacko AT, Kadzielski JJ, Appleton PT, Rodriguez EK. A novel methodology for the study of injury mechanism: ankle fracture analysis using injury videos posted on YouTube.com. J Orthop Trauma. 2010 Aug;24(8):477-82.
- Rodriguez EK, Kwon JY, Herder LM, Appleton PT. Correlation of AO and Lauge-Hansen classification systems for ankle fractures to the mechanism of injury. Foot Ankle Int. 2013; 34: 1516-1520.
- Somford MP, Wiegerinck JI, Hoornenborg D, van den Bekerom MPJ. Ankle fracture eponyms. JBJS 2013; 95(24): e198
- Tartaglione JP, Rosenbaum AJ, Abousayed M, DiPreta JA. Classifications in Brief: Lauge-Hansen Classification of Ankle Fractures. Clin Orthop Relat Res. 2015 Oct;473(10):3323-8
- Knipe H. Lauge-Hansen classification of ankle injury. Radiopaedia
- Eponymythology: Eponymous ankle and talus injuries. LITFL
eponymictionary
the names behind the name
Dr Josh Howard - wannabe future orthopod, finding myself in Australia | LinkedIn
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |