
![]()
Leo Rigler

Leo George Rigler (1896-1979) was an American radiologist.
Rigler was a prolific educator whose work influenced diagnostic imaging in the 20th century. Born in Minneapolis, Minnesota, he graduated MD from the University of Minnesota in 1920 and began training in radiology under Dr. Leroy Sante at St. Louis City Hospital. By 1933, Rigler had returned to Minnesota where he served as chief of radiology at both the University of Minnesota and Minneapolis General Hospital, positions he held until 1957.
Rigler was a pioneer in clinical radiology and published over 200 scientific articles and six textbooks, including the influential Outline of Roentgen Diagnosis (1938). He is eponymously remembered for multiple radiographic signs: the Rigler sign (pneumoperitoneum), Rigler triad (gallstone ileus), Rigler notch sign (bronchial carcinoma), and Hoffman-Rigler sign (left ventricular enlargement).
Rigler also held prominent community leadership roles and was the first Jewish president of the Radiological Society of North America. Additionally, he worked with the World Health Organization to improve radiology training in developing countries, including India, Iran, and Israel.
Biographical Timeline
- Born on October 16, 1896 in Minneapolis, Minnesota.
- 1920 – Received MD from the University of Minnesota.
- 1920s (early) – Internship at St. Louis City Hospital under radiologist Dr. Leroy Sante.
- 1927–1957 – Chief of Radiology at Minneapolis General Hospital.
- 1933–1957 – Chief of Radiology, University of Minnesota.
- 1934 – Became the 68th member certified by the American Board of Radiology.
- 1938 – Published Outline of Roentgen Diagnosis.
- 1941 – Described both the Rigler sign (radiographic sign of pneumoperitoneum) and Rigler triad (findings in gallstone ileus).
- 1955 – Introduced the Rigler notch sign related to bronchial carcinoma.
- 1957–1963 – Executive Director, Cedars of Lebanon and Sinai Hospitals, Los Angeles.
- 1963 – Appointed Professor of Radiology at UCLA and Director of the postgraduate training program.
- 1965 – Co-described the Hoffman-Rigler sign (for left ventricular enlargement).
- 1970 – Established the Leo G. Rigler Research Laboratory at UCLA.
- Died on October 25, 1979 in Los Angeles.
Medical Eponyms
Rigler sign (1941)
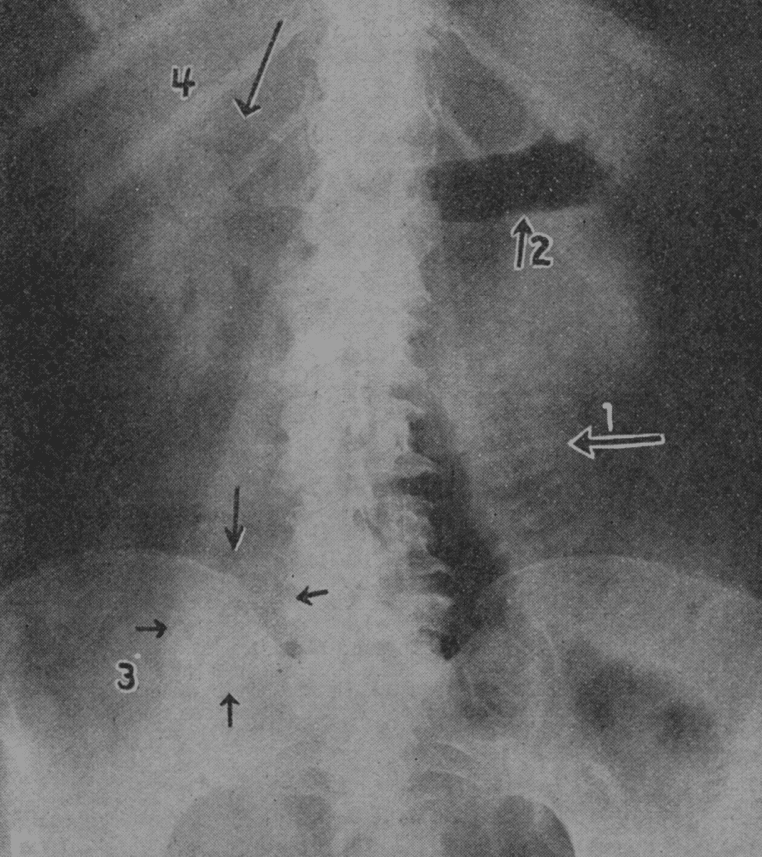
Rigler’s sign is a radiological indicator of pneumoperitoneum seen on supine abdominal X-ray. It appears when both sides of a bowel loop, the mucosal (inner) and serosal (outer) surfaces, are simultaneously outlined by gas. This occurs due to the presence of both intraluminal gas and free intraperitoneal air, rendering the normally invisible outer wall of the bowel visible.
1941 – Rigler described the pneumoperitoneum sign and emphasised that it would only be observed when large quantities of free gas were present.
A roentgenologic sign of pneumoperitoneum hitherto not reported or clearly defined is described. It consists of the demonstration of the outer as well as the inner bowel wall due to the accumulation of gas between the loops of bowel. It is of value because it can be observed in roentgenograms of the abdomen made in the supine position.
This sign may be the first evidence of the presence of pneumoperitoneum in cases in which such a condition is entirely unsuspected. Routine roentgenograms of the abdomen should be made at frequent intervals in all cases of obstruction of the gastro-intestinal tract which are being treated conservatively. Such films should always be examined for evidences of pneumoperitoneum because of the possibility of supervention of perforation without obvious clinical signs.
Rigler, Radiology 1941
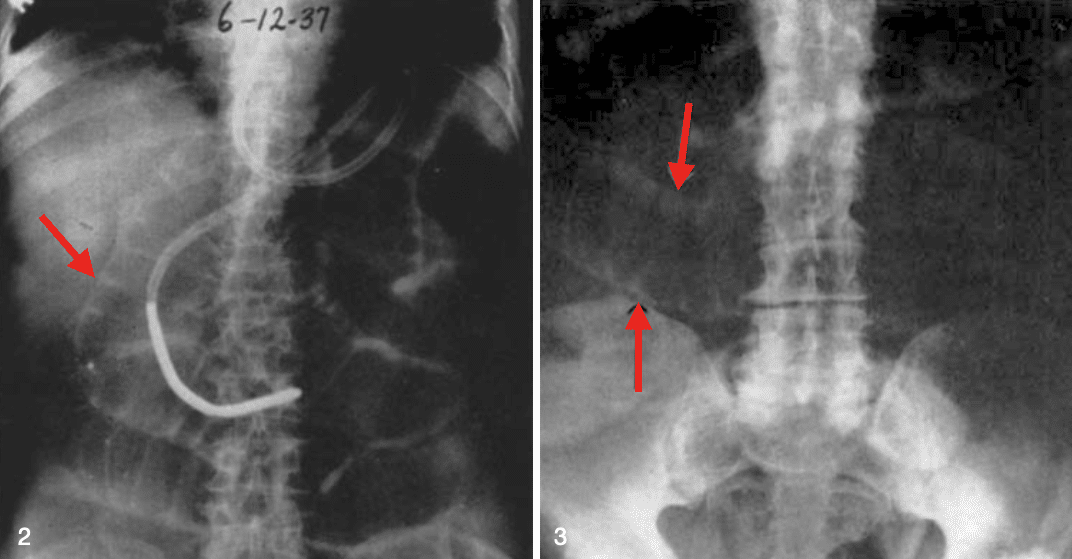
Fig. 3. Case of perforation of the colon with pneumoperitoneum; roentgenogram of abdomen, supine position. Note the distended loops of small bowel, both their inner and outer contours (arrows) being readily visible. Rigler 1941
Rigler triad (1941)
Rigler Triad refers to a classic set of radiographic features pathognomonic for gallstone ileus, a rare form of mechanical small bowel obstruction caused by the migration of a gallstone into the gastrointestinal tract via a biliary-enteric fistula
- Ectopic gallstone (often radiopaque and located in the intestinal lumen)
- Small bowel obstruction (evident as dilated small bowel loops)
- Pneumobilia (air in the biliary tree or gallbladder lumen)
1941 – Rigler described two cases, observed at autopsy, in which the manner of development of a choledochoduodenal and a cholecystoduodenal fistula could be demonstrated.
The specific signs which permit a roentgenologic diagnosis of this condition are evidences of dynamic ileus, presence of gas or contrast medium in the biliary tract and direct or indirect visualization of the calculus.
In 13 of 14 cases of gallstone obstruction in which roentgen examination was made, the exact diagnosis could have been made from the roentgenograms alone
Rigler, JAMA 1941
Rigler notch sign (1955)
Indentation in the border of a solid lung mass (thought to represent a nutrient/feeding vessel) and is suggestive of a bronchial carcinoma.
The sign is not pathognomonic of bronchial carcinoma being observed in other conditions, such as granulomatous infections. The sign as a differentiating utility is limited.
1955 – Rigler and Heitzman describe the notches pathologically and histologically.
In many histologic section of this small lesion shows an area of blood vessels surrounded by alveoli which is drawn into one side of the tumour. It is possible that the tumour has grown around this stalk, thus resembling the hilus of an organ.
Rigler and Heitzman, Radiology 1955
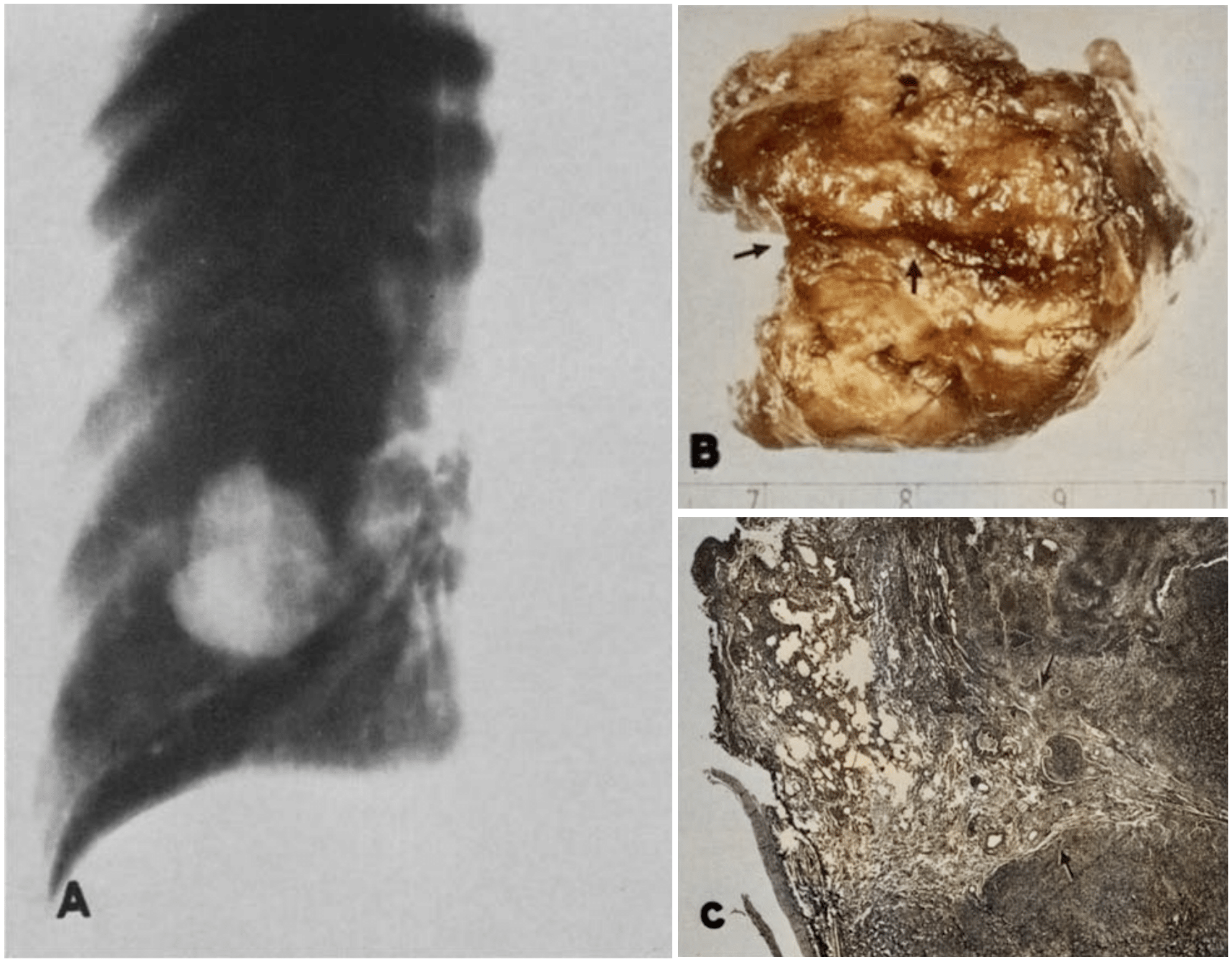
Fig. 8. Notch sign in a hypernephroma metastasis. A. Planigram showing large nodule in lung with marked indentation on lateral border, fairly characteristic of notch sign. B. Surgical specimen showing a deep groove (arrows) in the tumor corresponding to the notch. C. Microscopic section showing alveoli and blood vessels extending into the margin of the tumor. Radiology 1955
Hoffman-Rigler sign (1965)
A radiological sign used on the lateral chest X-ray to detect left ventricular enlargement (LVE). The sign is based on anatomical landmarks involving the left ventricle (LV) and inferior vena cava (IVC)
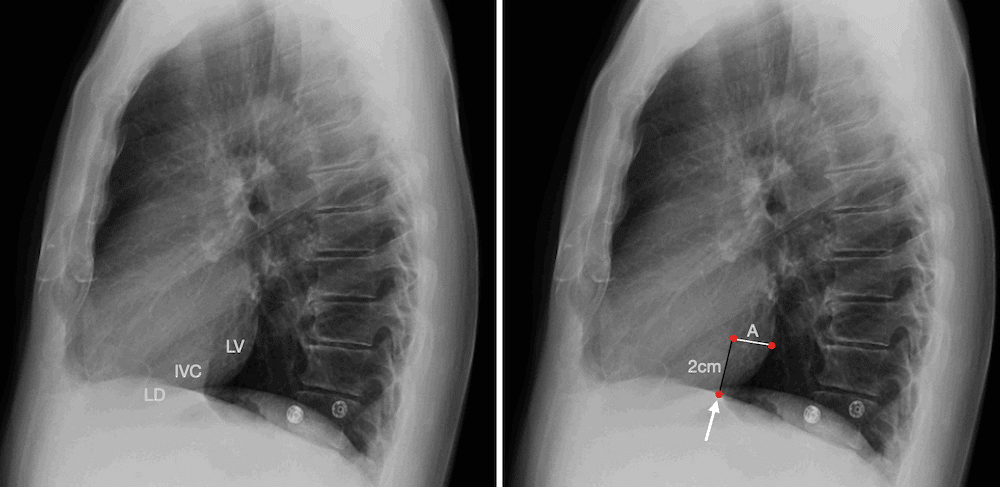
- A vertical line is drawn 2 cm cephalad from the intersection of the LV and IVC on the lateral projection.
- A second line is drawn posteriorly, parallel to the vertebral bodies.
- If the posterior border of the LV extends more than 1.8 cm beyond the IVC at this level, LVE is suggested.
1965 – Richard Bashefkin Hoffman (1937-2011) and Leo George Rigler (1896-1979) published their paper defining two measurements easily obtained from the lateral chest film and to determine their degree of efficacy in evaluating left ventricular size.
2008 – Serna et al evaluated the validity of the H&R sign against the echocardiographic LV end-diastolic diameter in 200 patients. They conclude that the Hoffman-Rigler sign is a valuable alternative in the evaluation of left ventricular enlargement when cardiac ultrasound is not readily available.
2016 – Spaziano et al investigated the sensitivity and specificity of the Hoffman-Rigler sign in a modern population. A sample of 145 patients with LV dilatation was matched for age and sex with 145
patients without LV dilatation. They found that while measurable in two-thirds of patients, the sign showed low diagnostic accuracy in modern populations.
Major Publications
- Rigler LG. Roentgen diagnosis of small pleural effusion. JAMA. 1931; 96(2): 104-108.
- Rigler LG. Outline of roentgen diagnosis. 1938
- Rigler LG. Spontaneous pneumoperitoneum: a roentgenologic sign found in the supine position. Radiology 1941; 37: 604–607 [Rigler sign]
- Rigler LG, Borman CN, Noble JF. Gallstone obstruction: pathogenesis and roentgen manifestations. JAMA. 1941; 117(21): 1753-1759. [Rigler Triad]
- Rigler LG. Outline of Roentgen diagnosis an orientation in the basic principles of diagnosis by the Roentgen method. 1943
- Rigler LG. The chest, a handbook of Roentgen diagnosis. 1946 [2e 1954]
- Rigler LG, Heitzman ER. Planigraphy in the differential diagnosis of the pulmonary nodule, with particular reference to the notch sign of malignancy. Radiology. 1955 Nov;65(5): 692-702. [Rigler notch sign]
- Rigler LG. A roentgen study of the evolution of carcinoma of the lung. J Thorac Surg. 1957 Sep; 34(3): 283-297
- Rigler LG. Functional roentgen diagnosis: anatomical image; physiological interpretation. Am J Roentgenol Radium Ther Nucl Med. 1959 Jul; 82(1): 1-24
- Hoffman R, Rigler L. Evaluation of the left ventricular enlargement in the lateral projection of the chest. Radiology 1965: 85: 93–100. [Hoffman-Rigler sign]
- Rigler LG. Bronchiolo-alveolar carcinoma of the lung: with report of new roentgenologic sign. XI International Congress of Radiology, Rome. Excerpta medica 1965
References
Biography
- Hodgson JR. Introduction of annual orator, Leo G. Rigler, M.D. Radiology. 1970 May;95(2):243-4.
- Memorial: Leo G. Rigler, 1896-1979. AJR Am J Roentgenol. 1980 Aug;135(2):421-2.
- Jacobson HG. In memoriam. Leo G. Rigler, M.D. 1896-1979. Radiology. 1980 Apr;135(1):247-8.
- Wangensteen OH. Tribute to a wonderful colleague, teacher, scientist, and humanist Leo G. Rigler. Minn Med. 1980 Nov;63(11):791-4.
- Lewicki AM. The Rigler sign and Leo G. Rigler. Radiology. 2004 Oct;233(1):7-12
- Heitzman ER. Leo G. Rigler, MD: a personal perspective. Radiology. 2004 Oct;233(1):13-14.
- Linton O. Leo G. Rigler. J Am Coll Radiol. 2005 Dec;2(12):1040-1
- Bibliography. Rigler, Leo G. (Leo George) 1896-1979. WorldCat Identities
Eponymous terms
- Levine MS, Scheiner JD, Rubesin SE, Laufer I, Herlinger H. Diagnosis of pneumoperitoneum on supine abdominal radiographs. AJR Am J Roentgenol 1991; 156(4): 731–735
- Freeman V, Mutatiri C, Pretorius M, Doubell A. Evaluation of left ventricular enlargement in the lateral position of the chest using the Hoffman and Rigler sign. Cardiovasc J S Afr. 2003 May-Jun;14(3):134-7
- Kanne JP, Rohrmann CA Jr, Lichtenstein JE. Eponyms in radiology of the digestive tract: historical perspectives and imaging appearances. Part I. Pharynx, esophagus, stomach, and intestine. Radiographics. 2006 Jan-Feb;26(1):129-42
- Maizlin ZV, Cooperberg PL, Clement JJ, Vos PM, Coblentz CL. People behind exclusive eponyms of radiologic signs (Part II). Can Assoc Radiol J. 2010 Feb;61(1):44-53.
Eponym
the person behind the name

BA, BM BCh University of Oxford, PgCert (Medical Education)University of Dundee. Aspiring medical physician with a particular interest in respiratory medicine, public health and medical education
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
