
![]()
LV function echocardiography
LV Function and Haemodynamic Assessment Echocardiography
SYSTOLIC FUNCTION
Global Function
- stroke volume: end-diastolic volume – end-systolic volume
- cardiac output:
Q = SV X HR
= (Aortic Area x V x Tej) x HR
Q = cardiac output
Aortic area = cross sectional area
V = velocity for each beat
Tej = time period during ejection
HR = heart rate
- ejection fraction: take two orthogonal views (apical four chamber and apical two chamber) ⇒ trace around endocardial border at the end of diastole and systole
EF = (EDV-ESV/EDV) x 100
(normal = 50-85%)
- fractional shortening: percentage change in LV internal dimensions between systole and diastole (normal 30-45%)
- preload: end-diastolic volume (if low think -> hypovolaemia, low SVR, severe AR or MR, VSD)
- afterload: end-systolic wall stress (rarely used in clinical practice)
- LV wall thickness: > 1.5cm = LVH, < 0.6cm = LV thinning
Regional Function
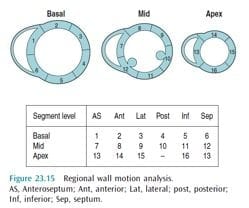
- 16 segments
- contractility: grades
1 = normal or hyperkinetic
2 = hypokinetic
3 = akinetic
4 = dyskinetic (paradoxical systolic motion)
5 = aneurysmal
DIASTOLIC FUNCTION
- relaxation requires energy (ATP)
- phases of relaxation = isovolumetric relaxation, early filling, diastasis (when LA passively fills LV and then stops), atrial contraction
- diastolic dysfunction = disorder of LV filling where LV is unable to fill to a normal LVEDV without an increase in end-diastolic pressure.
- m-mode ‘slow relaxation’ in motion of the anterior mitral valve leaflet.

- normal = E > A
- abnormal = A > E
- pseudonormal = E > A (LA dilated to compensated for lack of LV relaxation)
- restrictive = E >>> A
References and Links

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC