
![]()
Margaret Dix
Margaret Ruth Dix (1911-1991) was an English neuro-otologist.
Dix was a neuro-otologist whose work transformed the clinical evaluation of vertigo and vestibular disease. With Charles Skinner Hallpike, she co-devised the Dix–Hallpike manoeuvre, still the definitive bedside test for benign paroxysmal positional vertigo (BPPV).
Trained initially in surgery, Dix’s career was reshaped by personal adversity. During the Blitz of 1940 she sustained devastating facial injuries that ended her surgical ambitions, but under the pioneering care of Sir Archibald McIndoe she recovered and redirected her energies toward neuro-otology.
At Queen Square, within the MRC Otological Research Unit, she immersed herself in the study of inner ear disease and post-traumatic deafness in servicemen. Her landmark 1952 paper with Hallpike not only described the positional manoeuvre that bears their names but also set out a clinicopathological framework for vertigo that remains influential.
Biographical Timeline
- Born January 4, 1911 in Shifnal, Shropshire, UK the daughter of Shropshire rector Archibald William Dix (1877–1953) and Mary Ethel Briscoe (1873–1948)
- Attended Sherborne School for Girls and Royal Free School of Medicine in London.
When asked why she chose a medical career, Margaret would reply: “Because a woman cannot be a clergyman!”
- 1937 – MBBS, Royal Free Hospital School of Medicine. Commenced surgical training. Her supervisors recognised her competence and allowed her to perform tonsillectomy procedures.
- 1940 – Injured in Blitz, ending surgical career. Margaret suffered facial disfigurement, a torn eardrum and fragments of glass lodged in her eyes which prevented her from continuing as a surgeon.
- 1945 – Joined MRC Otological Research Unit, National Hospital, Queen Square. Alongside otologist Charles Skinner Hallpike, she studied and practiced neuro-otology and carried out research on deafness in ex-servicemen.
- 1952 – Co-authored the landmark paper on benign paroxysmal positional vertigo (BPPV), describing the Dix–Hallpike manoeuvre
- 1957 – Earned Doctor of Medicine (MD)
- 1965 – Appointed Honorary Consultant, National Hospital, and worked there until her retirement
- 1976 – Retired after more than 30 years in vestibular research; had published over 100 scientific papers.
- 1980 – Awarded Norman Gamble Research Prize
- December 9, 1991 aged 80
Medical Eponyms
Dix-Hallpike Test (1952)
The Dix–Hallpike manoeuvre remains the gold-standard bedside test for diagnosing benign paroxysmal positional vertigo (BPPV). By provoking vertigo and nystagmus through rapid changes in head position, it distinguishes peripheral vestibular disease from central causes of dizziness. Its enduring value lies in its simplicity, reproducibility, and ability to reveal characteristic patterns of nystagmus associated with posterior semicircular canal dysfunction.
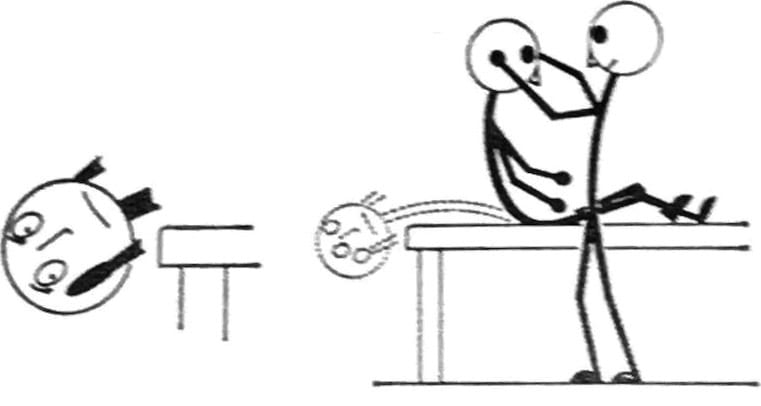
In their landmark 1952 paper, Margaret Ruth Dix and Charles Skinner Hallpike provided the first detailed description of what they termed the Lagerungs (positioning) manoeuvre, writing:
The patient is laid supine upon a couch with his head just over its end. The head is then lowered some 30 degrees below the level of the couch and turned some 30 degrees to 45 degrees to one side. In taking up this position, the patient is first seated on the couch with the head turned to one side and the gaze fixed upon the examiner’s forehead. The examiner then grasps the patient’s head firmly between his hands and briskly pushes the patient back into the critical position.
Dix and Hallpike, 1952
From their prospective study of 100 patients, Dix and Hallpike not only established the clinical hallmarks of BPPV but also coined the term “positional vertigo of the benign paroxysmal type”. Their method soon became widely adopted, and by the late 20th century it was universally referred to as the Dix–Hallpike manoeuvre, enshrining both investigators’ names in the history of modern neuro-otology.
Dix–Hallpike Manoeuvre: Original vs. Modern Interpretation
| Aspect | Dix & Hallpike, 1952 (Original Description) | Modern Clinical Criteria |
|---|---|---|
| Patient position | “The patient is seated on the couch with the head turned 30–45° to one side, gaze fixed on the examiner’s forehead… The examiner then briskly pushes the patient back, so the head lies 30° below horizontal, over the end of the couch.” | Patient starts sitting upright; head is rotated 45° toward test side; patient rapidly lowered to supine with head hanging 20–30° below horizontal. |
| Provocation | Rapid change in head position relative to gravity (Lagerungs manoeuvre). | Same principle; diagnostic for posterior canal BPPV. |
| Nystagmus observed | Rotatory nystagmus beating toward the undermost ear, after a short latency, with fatigability on repetition. | Posterior canal: torsional upbeat nystagmus with 2–15 sec latency; fatigues with repetition; reversal on sitting up. |
| Interpretation | Described as “positional vertigo of the benign paroxysmal type.” | Standard diagnostic test for BPPV; allows canal-specific localisation (posterior > lateral > anterior). |
| Clinical impact | First systematic clinical–physiological correlation of vertigo with head positioning; established reproducible manoeuvre for research and practice. | Remains the gold standard bedside test; used worldwide; essential for guiding repositioning treatments (Epley, Semont, etc.). |
Key Medical Contributions
Peep-Show technique for pure tone audiometry (1947)
Diagnosing deafness in children under the age of six is challenging because pure tone audiometry sounds are meaningless to young children and require explanation beyond their understanding.
Dix and Hallpike aimed to solve this problem by designing an apparatus called the “Peep-Show”, to enable young children to reliably respond to sounds. The apparatus consisted of a lamp and loudspeaker, and a box containing hidden pictures.
The test was devised to overcome the main difficulties in applying audiometric methods to young children — lack of co-operation and failure to understand instructions… the child is rewarded by seeing a picture light up in the peep-show, and once conditioned, will respond reliably to sound alone
Dix and Hallpike, 1947
The tester shows the child that when the lamp and loudspeaker activate, the child can make the pictures appear by pressing a switch. After the child does this several times, the lamp is removed, and now only the loudspeaker activates.
- A child who can hear the sound, will still press the switch when the sound occurs, to reveal the picture.
- A child who cannot hear the sound, will not.
The test allowed deafness to be identified and quantified in young children, enabling special education to commence at an early age.
Caloric Test (Cawthorne, Dix & Hallpike, 1956)
The caloric test is a cornerstone of vestibular assessment, based on Bárány’s discovery (1906) that irrigation of the ear canal with warm or cold water induces convection currents in the endolymph of the horizontal semicircular canal, generating nystagmus.
Dix and Hallpike, working with Terence Cawthorne and others at Queen Square, refined this method into a reproducible, patient-friendly protocol using water at 30°C and 44°C, each equidistant from body temperature.
In practice, we employ water at 30 °C and 44 °C, which are respectively 7° below and 7° above body temperature… The essential features of the method are its reproducibility, its ability to indicate the sensitivity of the labyrinths, and its value in demonstrating directional preponderance.
Cawthorne et al, 1956
Their work in the 1940s–50s demonstrated not only labyrinthine sensitivity but also “directional preponderance,” a pathological asymmetry of vestibular responses, sometimes due to central lesions such as infarcts of the posterior inferior cerebellar artery. They showed that caloric testing could distinguish between peripheral and central causes of vertigo.
Controversies
Date of Birth Anomaly
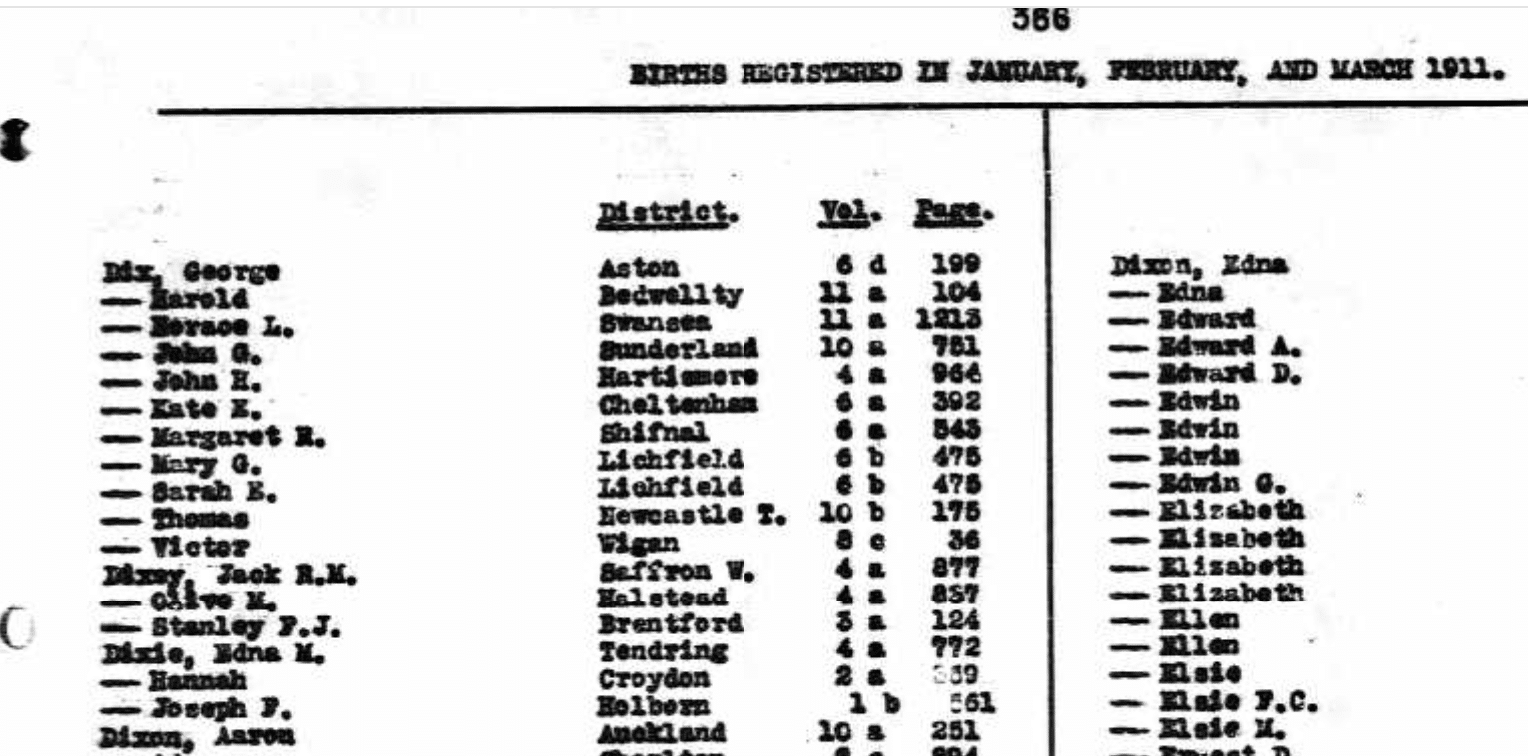
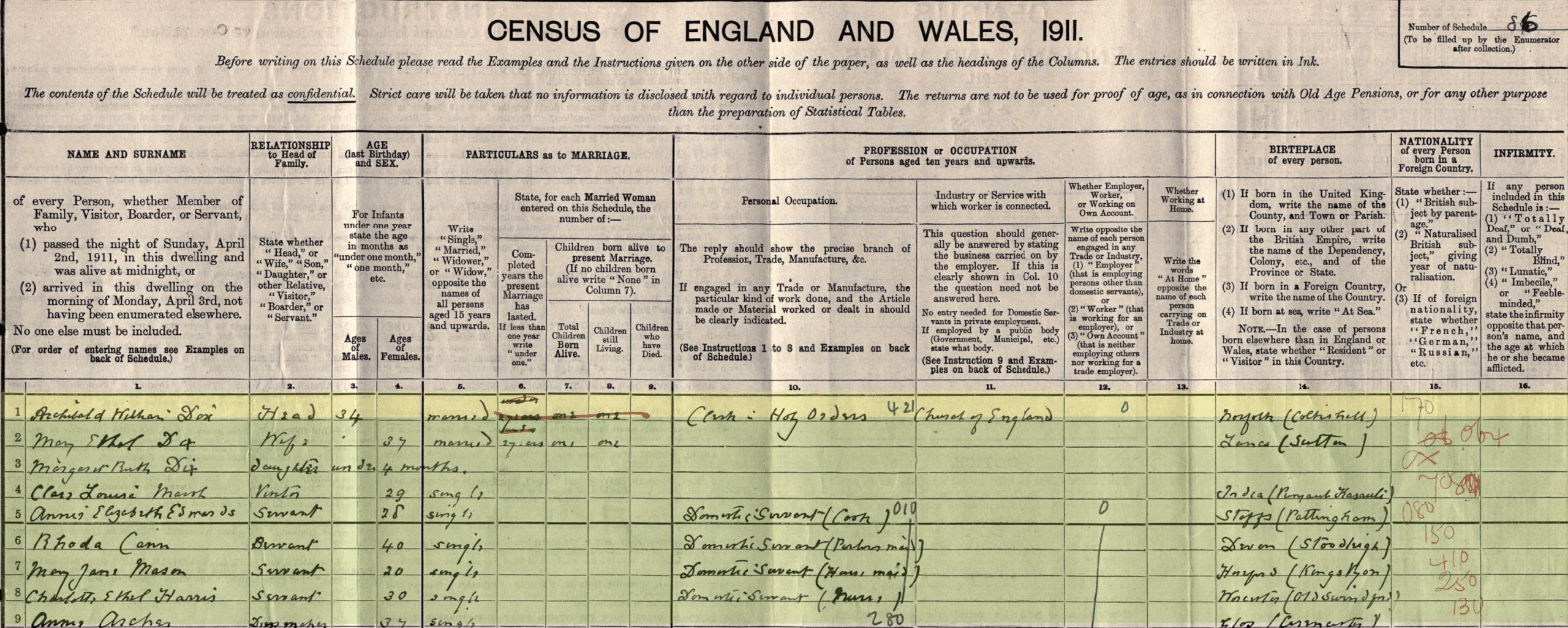
Margaret Ruth Dix’s birth year has long been confused in the literature. Many secondary sources, including obituaries and reference works, list 1902 as her date of birth. However, multiple pieces of primary documentation demonstrate conclusively that she was born in early 1911:
- Birth Registry: The official England and Wales birth index records Margaret R. Dix registered in Shifnal, Shropshire, Jan–Mar 1911
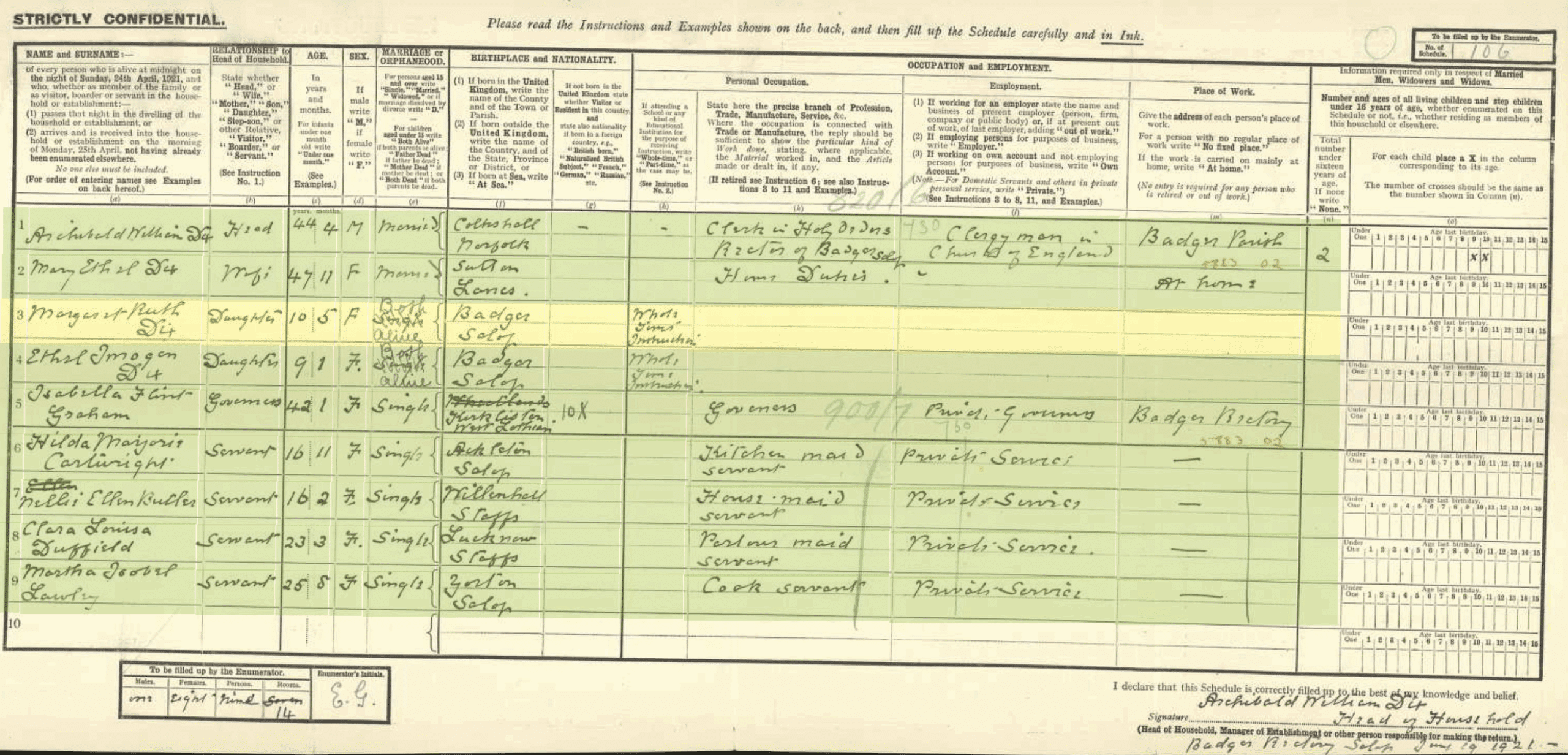
- 1911 Census: Taken on April 2, 1911, lists Margaret Ruth Dix as aged 0 years, 3 months, living with her parents Archibald William Dix (rector of Badger) and Mary Ethel Dix, Confirmed in 1921 census as 10 years of age
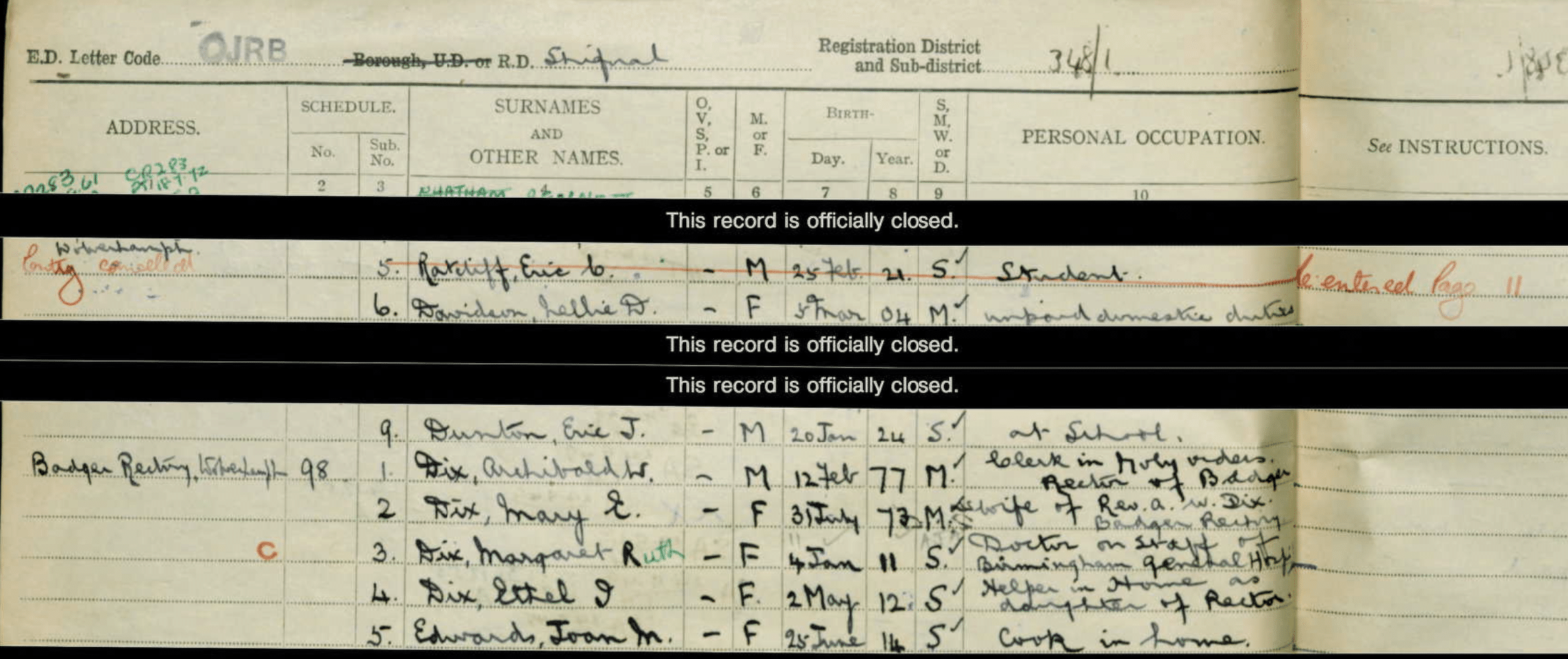
- 1939 Register: Records her date of birth as January 4, 1911, while she was working as a doctor at Birmingham General Hospital
- 1991 Obituary: The Daily telegraph has hwer age at death as 80 years, in keeping with birth year of 1911
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The persistence of the 1902 date likely stems from an early misprint in biographical notices that was copied forward into later works.
Conclusion: Margaret Ruth Dix was born January 4, 1911 and not 1902. This correction aligns all surviving primary documents and resolves the longstanding discrepancy.
Major Publications
- Dix MR, Hallpike CS. The peep-show: a new technique for pure-tone audiometry in young children. Br Med J. 1947; 2(4531): 719-23. [Peep-Show technique]
- Dix MR, Hallpike CS. The pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Ann Otol Rhinol Laryngol. 1952; 61(4): 987-1016. [Dix-Hallpike Test]
- Dix MR, Hallpike CS. The pathology symptomatology and diagnosis of certain common disorders of the vestibular system. Proc R Soc Med. 1952; 45(6): 341-54 [Dix-Hallpike Test]
- Cawthorne T, Dix MR, Hallpike CS, Hood JD The investigation of vestibular function. Br Med Bull. 1956;12(2):131-142.
References
Biography
- DIX, Margaret Ruth. The Daily Telegraph, Wed, 11 Dec 1991: 20
- Ramirez-Gil LS, Espinosa-Arce CB. From Injury to Innovation: Margaret Dix’s Pioneering Work in Neuro-Otology. Cureus. 2024 Nov 5;16(11):e73094
- Margaret R Dix. Portraits – Queen Square archives
- Margaret Ruth Dix. Plarr’s Lives of the Fellows
Eponymous terms
- Lanksa DJ, Remler B. Benign paroxysmal positioning vertigo: classic descriptions, origins of the provocative positioning technique, and conceptual developments. Neurology 1997;48;1167.
- Maranhão-Filho P, Nandi R, Maranhão ET. Margaret Dix, Charles Hallpike and the ‘Lagerungs’ Manoeuvre. Arq Neuropsiquiatr. 2018 Aug;76(8):563-565
- Baloh RW. Vertigo: Five Physician Scientists and the Quest for a Cure. Oxford University Press. 2016: 187
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |

MBBCh Cardiff University School of Medicine. BSC (Hons) Medical Microbiology Leeds University. I am a current ED RMO at the Sir Charles Gairdner Hospital in Perth hoping to pursue a career in ENT surgery.