
![]()
SNRI toxicity
SNRIs or Selective serotonin and noradrenaline reuptake inhibitors are mainly in the form of venlafaxine and desvenlafaxine. Venlafaxine in overdose can be potentially life threatening, causing seizures and cardiotoxicity. There is less experience with desvenlafaxine and so the management and risk assessment for this drug is currently extrapolated from venlafaxine, although it is likely it has less toxic effects.Toxic Mechanism:
They are potent serotonin and noradrenaline reuptake inhibitors with rate-dependent sodium channel blocking activity.
Toxicokinetics (venlafaxine):
- Well absorbed but extensive first pass metabolism resulting in a bioavailability of 50%
- Peak plasma levels 6 – 8 hours
- Large Volume of distribution 5 – 7 L/kg
- Hepatic metabolism to water soluble and less active metabolites
- Elimination half life is approximately 15 hours
Resuscitation:
- Seizures: IV benzodiazepines incrementally dosed every 5 minutes to effect (aiming for gentle sedation and a heart rate falling towards 100 beats per minute).
- Check the patient is not in a dysrhythmia
- Can be managed with benzodiazepines (varying doses in the textbooks, easy method is 0.1mg/kg IV for lorazepam (max 4mg) / midazolam (max 10mg) / diazepam (max 10mg). Or…
- Lorazepam 0.1mg/kg max 4mg
- Diazepam 0.15mg/kg max 10mg
- Midazolam 0.2mg/kg max 10mg
- Hyperthermia (>39.5 degrees centigrade): This is a feature of severe serotonin toxicity and needs immediate control to prevent multi organ failure. Treatment is with paralysis, intubation, ventilation and cooling.
Risk Assessment
- Dose related risk assessment of Venlafaxine:
- <1.5 grams Risk of seizures < 5%
- <3 grams Risk of seizures 10%
- >3 grams Risk of seizures > 30%
- >4.5 grams Risk of seizures approaches 100%, hypotension, minor QRS and QT prolongation
- >7 grams Risk of seizures 100%, hypotension, left ventricular dysfunction
- Seizures: Can be delayed up to 16 hours
- Serotonin toxicity: High risk of serotonin toxicity if other serotinergic agents have been ingested irrespective of the venlafaxine dose.
- Children: An accidental ingestion go <12.5 mg/kg is not associated with significant symptoms.
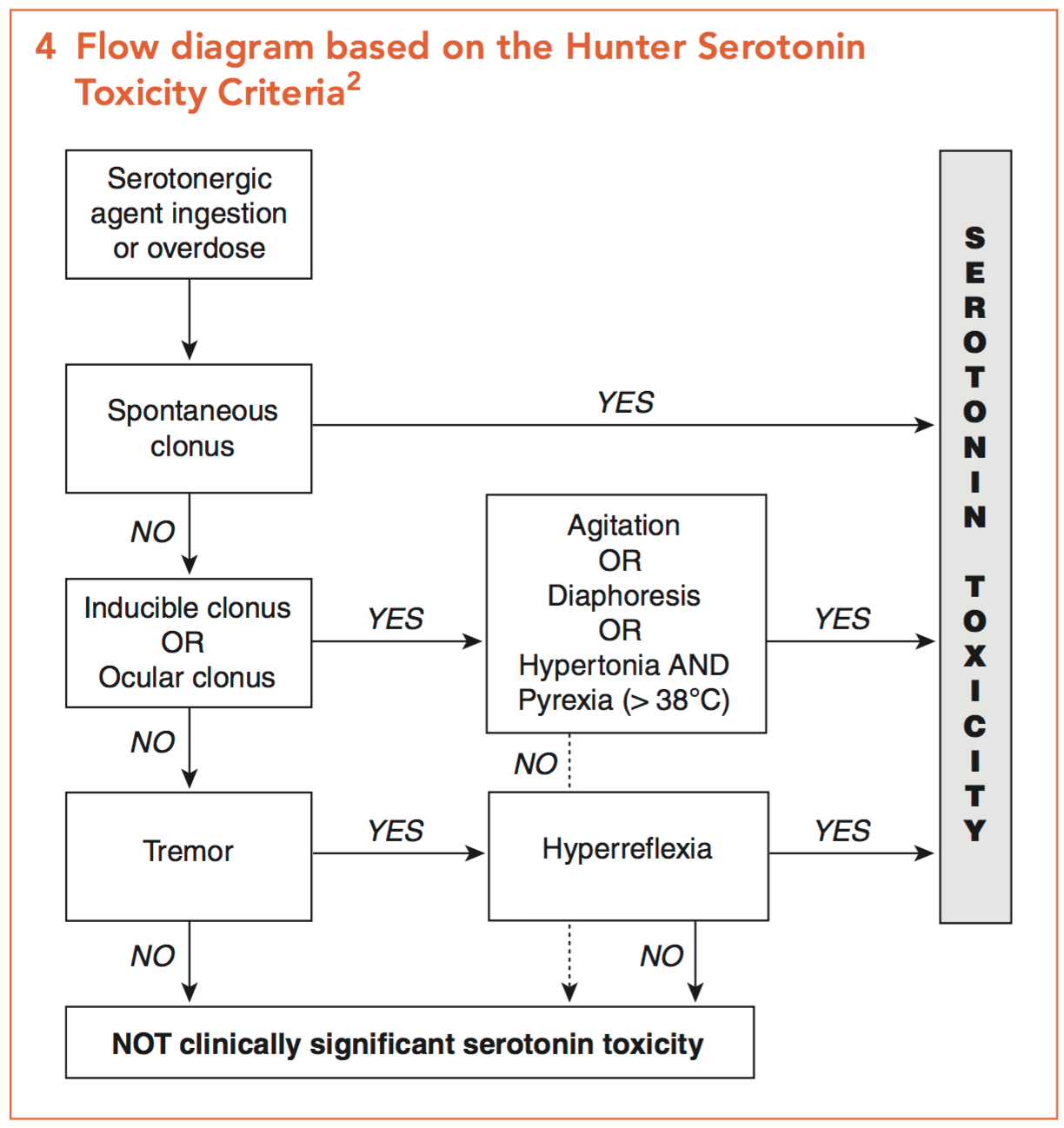
Serotonin syndrome aide memoire
My quick easy method: Fever M.A.N. = Fever plus Mental state changes, Autonomic instability and Neuromuscular changes.
- Clinical features:
- Can be delayed for 12 – 16 hours post ingestion (including hypotension and left ventricular dysfunction)
- Dysphoria
- Anxiety
- Mydriasis
- Sweating
- Tremor
- Clonus
- Tachycardia up to 160 beats per minute
- Hypertension
- Seizures are often short lived and self limiting
- Coma is not a feature of venlafaxine toxicity therefore if present other causes must be sought
- Rhabdomyolysis and hypoglycaemia have been reported in massive overdose
- Toxicity usually resolves within 24 hours
Supportive Care
- Agitation and tachycardia: Increasing anxiety, sweating, tremor, tachycardia and mydriasis may herald the onset of seizures. Titrated doses of benzodiazepines are effective e.g. diazepam 2.5 – 5 mg every 5 minutes IV until gentle sedation is achieved and a heart rate falls towards 100 beats per minute is considered safe.
Investigations
- Screening: 12 lead ECG, BSL, Paracetamol level
- Specific:
- For ingestions <4.5 grams cardiac monitoring is not required after the first 6 hours provided the QRS and QT are normal or at baseline. For >4.5 grams cardiac monitoring must remain for at least 12 hours.
- CK to detect and monitor rhabdomyolysis
Decontamination:
- 50 grams of activated charcoal can be given to cooperative patients within 2 hours post ingestion who have ingested >4.5 grams of venlafaxine or desvenlafaxine.
- Activated charcoal is contraindicated in the awake patient with a more delayed presentation or one with symptoms due to the risk of seizures.
Enhanced Elimination
- Not clinically useful.
Antidote
- None available for SNRIs per se.
- Serotonin toxicity: There maybe a role for serotonin antagonists for mild to moderate serotonin toxicity refractory to benzodiazepines. If the patient has severe toxicity aggressive supportive care including cooling, intubation, ventilation and neuromuscular paralysis will be necessary – do not use the specific serotonin antagonists below in this situation.
- Cypoheptadine: Antihistamine with anti-serotinergic effects, can be given orally or via a nasogastric tube. 8mg TDS if there is a positive response after the first dose. Stop after 24 hours.
- Olanzapine: 5 – 10 mg sublingual
- Chlorpromazine: 25 – 100 mg in 100ml of 0.9% saline over 60 minutes. However, adverse effects are common including increased sedation, orthostatic hypotension and anticholinergic side effects.
Disposition
- All patients must be observed for a minimum of 16 hours with an IV in situ. They are medically cleared when symptom free. Beware some patients may have delayed seizures up to 24 hours later.
- Severe venlafaxine intoxication or serotonin toxicity require ICU care
Additional Resources and References:
Additional Resources:
- CCC – Serotonin syndrome
- CCC – Hyperthermia associated toxidromes
- Tox conundrum 024 – Serotonin toxicity
- Tox conundrum 025 – Toxidrome challenge
References:
- Howell C, Wilson AD, Waring WS. Cardiovascular toxicity due to venlafaxine poisoning in adults: a review of 235 consecutive cases. British Journal of Clinical Pharmacology 2007; 64(2):192-197.
- Isbister GK. Electrocardiogram changes and arrhythmias in venlafaxine overdose. British Journal of Clinical Pharmacology 2009; 67(5):572-576.
- Kumar VV et al. The effect of decontamination procedures on the pharmacokinetics of venlafaxine in overdose. Clinical Pharmacology and Therapeutics 2009; 27:911-915
- Rotella JA, Taylor DM, Wong A, Greene SL. Accuracy of QT interval measurements on electrocardiographs displayed on electronic ‘smart’ devices. Emergency Medicine Australia 2016; 28:187-192
- Whyte IM, Dawson AH, Buckley NA. Relative toxicity of venlafaxine and selective serotonin reuptake inhibitors in overdose compared to tricyclic antidepressants. Quarterly Journal of Medicine 2003; 96(5): 369-374.

Toxicology Library
DRUGS and TOXICANTS
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.
