![]()
SSRI toxicity
SSRIs or Selective serotonin reuptake inhibitors are common in overdose and usually follow a benign course. Serotonin toxicity occurs in a minority but is more common with co-ingestant agents with serotonergic action. Citalopram (>600 mg) and escitalopram (>300 mg) are unique in their ability to cause dose dependent QT prolongation and a risk of torsades de points.
Toxic Mechanism:
Simple mechanism, they solely enhance the central serotonergic neurotransmission by inhibiting serotonin reuptake. Exactly what they say in the name.
Toxicokinetics:
- Good oral absorption
- Highly protein bound
- Large Volume of distribution 12 – 97L/kg
- Hepatic metabolism to water soluble and less active metabolites
- Elimination half life is approximately 24 hours
Resuscitation:
- Seizures: IV benzodiazepines incrementally dosed every 5 minutes to effect.
- Check the patient is not in a dysrhythmia
- Can be managed with benzodiazepines (varying doses in the textbooks, easy method is 0.1mg/kg IV for lorazepam (max 4mg) / midazolam (max 10mg) / diazepam (max 10mg). Or…
- Lorazepam 0.1mg/kg max 4mg
- Diazepam 0.15mg/kg max 10mg
- Midazolam 0.2mg/kg max 10mg
Risk Assessment
- Seizures: Occur in <4% of patients and are more likely with citalopram.
- Torsades de pointes: Very rare. QT prolongation occurs with >600 mg of citalopram and >300 mg of escitalopram.
- Serotonin toxicity: Usually mild symptoms and only in 20% of patients, usually lasts <12 hours. Co-ingestion with other serotonergic agents greatly increases the risk of serotonin toxicity. Minor symptoms are usually present within 4 hours and have resolved within 12 hours.
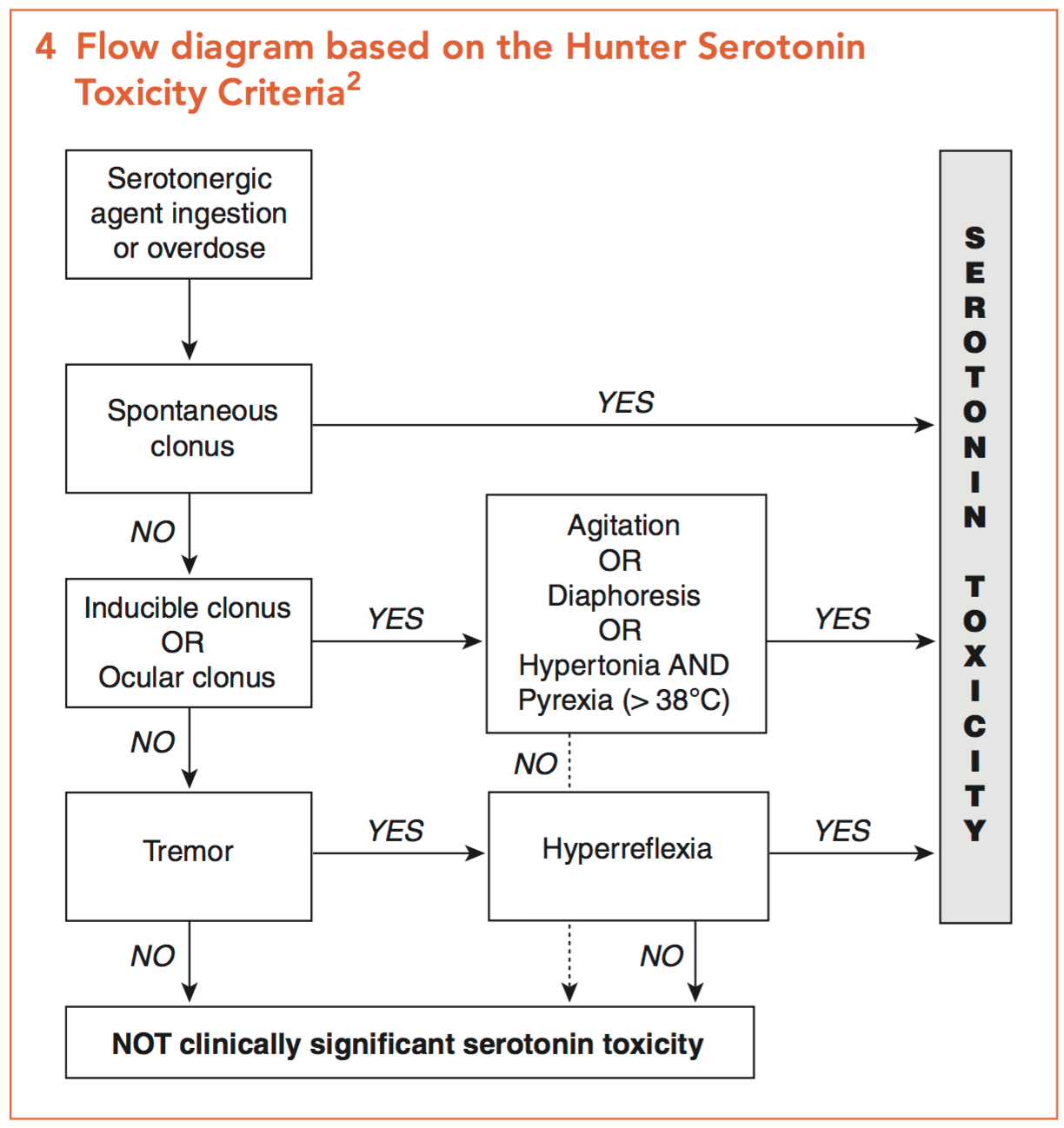
Serotonin syndrome aide memoire
My quick easy method: Fever M.A.N. = Fever plus Mental state changes, Autonomic instability and Neuromuscular changes.
- Children: Ingestion of up to 3 tablets is benign. Referral to hospital is only required in a larger ingestion of if they become symptomatic.
Supportive Care
- Agitation and tachycardia: Increasing anxiety, sweating, tremor, tachycardia and mydriasis may herald the onset of seizures. Titrated doses of benzodiazepines are effective e.g. diazepam 2.5 – 5 mg every 5 minutes IV until gentle sedation is achieved and a heart rate falls towards 100 beats per minute is considered safe.
Investigations
- Screening: 12 lead ECG, BSL, Paracetamol level
- Continuous cardiac monitoring is required for citalopram (>600 mg) and escitalopram (>300mg) for at least 8 hours. If citalopram (>1000 mg) and escitalopram (>500 mg) has been ingested then at least 12 hours of cardiac monitoring is required.
- The QT should be measured on the QT nomogram (not using the Bazett formula in toxicology). Technically the average QT of 6 leads should be plotted on the nomogram but recent evidence would indicate lead V2 is the most accurate if only one lead is to be used.
Decontamination:
- Alert and cooperative patients who have ingested >600 mg citalopram or >300 mg escitalopram may have 50 g of activated charcoal within 4 hours after overdose. Giving charcoal has to be weighed against the risk of seizures and aspiration.
- Overdose with other SSRIs does not warrant activated charcoal as the clinical course is more benign
Enhanced Elimination
- Not clinically useful.
Antidote
- None available for tramadol per se.
- Serotonin toxicity: There maybe a role for serotonin antagonists for mild to moderate serotonin toxicity refractory to benzodiazepines. If the patient has severe toxicity aggressive supportive care including cooling, intubation, ventilation and neuromuscular paralysis will be necessary – do not use the specific serotonin antagonists below in this situation.
- Cypoheptadine: Antihistamine with anti-serotonergic effects, can be given orally or via a nasogastric tube. 8mg TDS if there is a positive response after the first dose. Stop after 24 hours.
- Olanzapine: 5 – 10 mg sublingual
- Chlorpromazine: 25 – 100 mg in 100ml of 0.9% saline over 60 minutes. However, adverse effects are common including increased sedation, orthostatic hypotension and anticholinergic side effects.
Disposition
- Most children can be observed at home unless symptomatic
- Citalopram (>600 mg) and escitalopram (>300mg) requires monitoring for at least 8 hours
- Citalopram (>1000 mg) and escitalopram (>500 mg) requires monitoring for at least 12 hours
- All other patients require 6 hours of observation and if they are asymptomatic at the end of this time with a normal 12-lead ECG they can be medically cleared
- Symptomatic patients require 12-24 hours of monitoring and supportive care and can be medically cleared once asymptomatic with a normal 12-lead ECG
- Patient who develop severe serotonin toxicity require HDU/ICU care
Additional Resources and References:
Additional Resources:
- CCC – Serotonin syndrome
- CCC – Hyperthermia associated toxidromes
- Tox conundrum 024 – Serotonin toxicity
- Tox conundrum 025 – Toxidrome challenge
References:
- Hayes BD et al. Comparison of toxicity of acute overdose with citalopram and escitalopram. Journal of Emergency Medicine 2010; 39(1):44-48
- Isbister GK et al. Relative toxicity of selective serotonin reuptake inhibitors (SSRIs) in overdose. Clinical Toxicology 2004; 42(3): 277-285.
- Isbister GK, Friberg LE, Duffull SB. Application of pharmacokinetic-pharmacodynamic modelling in the management of QT abnormalities after citalopram overdose. Intensive Care Medicine 2006; 32(7):1060-1065.
- Isbister GK et al. Activated charcoal decreases QT prolongation after citalopram overdose. Annals of Emergency Medicine 2008; 52(1):86-87
- Isbister GK. Risk assessment of drug-induced QT prolongation. Australian Prescriber 2015; 38(1):20-24
- Jimmink A et al. Clinical Toxicology of citalopram after acute intoxication with the sole drug or in combination with other drugs: overview of 26 cases. Therapeutic Drug Monitoring 2008; 30(3):365-71.
- Rotella JA, Taylor DM, Wong A, Greene SL. Accuracy of QT interval measurements on electrocardiographs displayed on electronic ‘smart’ devices. Emergency Medicine Australia 2016; 28:187-192
- Van Gorp F, Whyte IM, Isbister GK. Clinical and ECG effects of escitalopram overdose. Annals of Emergency Medicine 2009: 54(3): 404-408.
- Van Gorp F, Dufful S, Hackett LP, Isbister GK. Population pharmacokinetics and pharmacodynamics of escitalopram in overdose and the effect of activated charcoal. British Journal of Clinical Pharmacology 2011; 73:402-410

Toxicology Library
DRUGS and TOXICANTS
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.