
![]()
Staph Sepsis Acidosis
aka Metabolic Muddle 004
You are asked to review a 73 year old lady who is in hospital for treatment of septic arthritis affecting a prosthetic right hip joint inserted 5 years earlier. The joint has been washed out and debrided twice, and she is receiving IV flucloxacillin and meropenem following culture of a methicillin-sensitive Staphylococcus aureus. She is on regular paracetamol for pain. Unfortunately, she has continued to deteriorate and now has bilateral patchy infiltrates on her chest x-ray.
Vital signs: Heart rate 115/min, BP 105/55 mmHg, RR 35/min, SpO2 100% on FiO2 0.5 and GCS 12.
Her UEC and ABG results are shown:

Modification of Case 1; Dempsey et al, 2000
Questions
Q1. What is the anion gap?
Answer and interpretation
Remember that:
- anion gap = [Na] – ([HCO3] + [Cl])
- normal anion gap is 2-10 mEq/L
In this case the anion gap is high:
- 142 – (8 + 104) = 30 mEq/L
Q2. Describe the acid-base disturbance.
Answer and interpretation
Severe acidemia (pH 7.15) resulting from a high-anion gap metabolic acidosis (HAGMA) with incomplete respiratory compensation.
Incomplete respiratory compensation may due to the presence of bilateral pulmonary infiltrates, exhaustion or obtundation.
Q3. What is the likely cause of the primary acid-base disturbance? How would you confirm it?
Answer and interpretation
Remember the causes of HAGMA?
- CAT-MUDPILES – see Metabolic Muddle #003
Given that the lactate and ketones are normal the most likely cause is:
- pyroglutamic acidemia (aka 5-oxoprolinemia)
This can be confirmed by performing a metabolic screen for urinary organic acids. Blood levels may be required if the patient is anuric. An elevated level of pyroglutamic acid confirms the diagnosis.
Q4. What is the underlying biochemical mechanism?
Answer and interpretation
…Skip this one if you’re biochemically challenged…
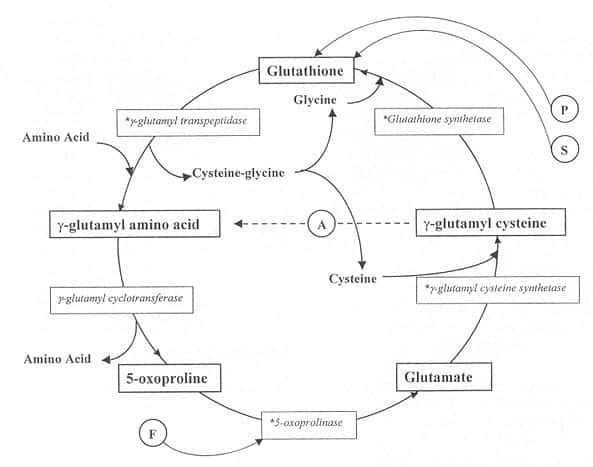
5-oxoproline (aka pyroglutamic acid) is produced from γ-glutamyl cysteine by the enzyme γ-glutamyl cyclotransferase. This enzyme’s activity increases when glutathione levels are low, due to a loss of feedback inhibition from glutathione.
Thus the accumulation of pyroglutamic acid is thought to be due to depletion of the glutathione, particularly when glutathione synthetase is inhibited. Decreased activity of 5-oxoprolinase, which breaks down pyroglutamic acid, may also play a role.
Check out the γ-glutamyl cycle to see how this all links up:
Q5. What factors may contribute to this?
Answer and interpretation
Factors that may contribute to pyroglutamic acidemia include:
- Drugs:
- paracetamol — depletion of glutathione by its metabolite N-acetyl-p-benzoquinoneimine (aka NAPQI)
- flucloxacillin — inhibition of 5-oxoprolinase
- vigabatrin
- Severe sepsis:depletion of hepatic glutathione pools due to oxidative stress from stimulated leukocytes, reperfusion of ischemic tissue, or endotoxemia
- Organ dysfunction — hepatic, renal
- Other — malnutrition, pregnancy
- Congenital enzyme deficiencies — e.g. glutathione synthetase deficiency (mental retardation, hemolytic anemia and metabolic acidosis)
Q6. What is the appropriate management?
Answer and interpretation
Management options include:
- Stop or change exacerbating medications
- Treatment or removal of source of sepsis (e.g. plan removal of hip prosthesis in this case)
- Provide appropriate ICU-level management of severe sepsis and organ support — intubation and ventilation as required, hemofiltration for renal failure, etc.
- N-acetylcysteine — may help replenish glutathione stores.
- Sodium bicarbonate — may or may not be beneficial in severe HAGMA.
References
- Dempsey GA, Lyall HJ, Corke CF, Scheinkestel CD. Pyroglutamic acidemia: a cause of high anion gap metabolic acidosis. Critical care medicine, 2000;28 (6):1803-7 PMID: 10890623
- Mizock BA, Mecher C. Pyroglutamic acid and high anion gap: looking through the keyhole? Critical care medicine, 2000;28 (6), 2140-1 PMID: 10890683
- Peter JV, Rogers N, Murty S, Gerace R, Mackay R, Peake SL. An unusual cause of severe metabolic acidosis. The Medical journal of Australia, 2006;185 (4), 223-5 PMID: 16922670
CLINICAL CASES
Metabolic Muddle
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
