
![]()
Stressed and branching out
aka Ophthalmology Befuddler 021
A 24 year-old medical student presents to the emergency department with 2 days of superficial left eye pain, mild redness, tearing and mild photophobia. She has a history of cold sores and has been stressed out by exams recently.
Prior to applying topical anesthesia, you checked corneal sensation, which was decreased.
Slit lamp examination reveals this:

Questions
Q1. What is the likely diagnosis?
Answer and interpretation
Herpes simplex keratitis
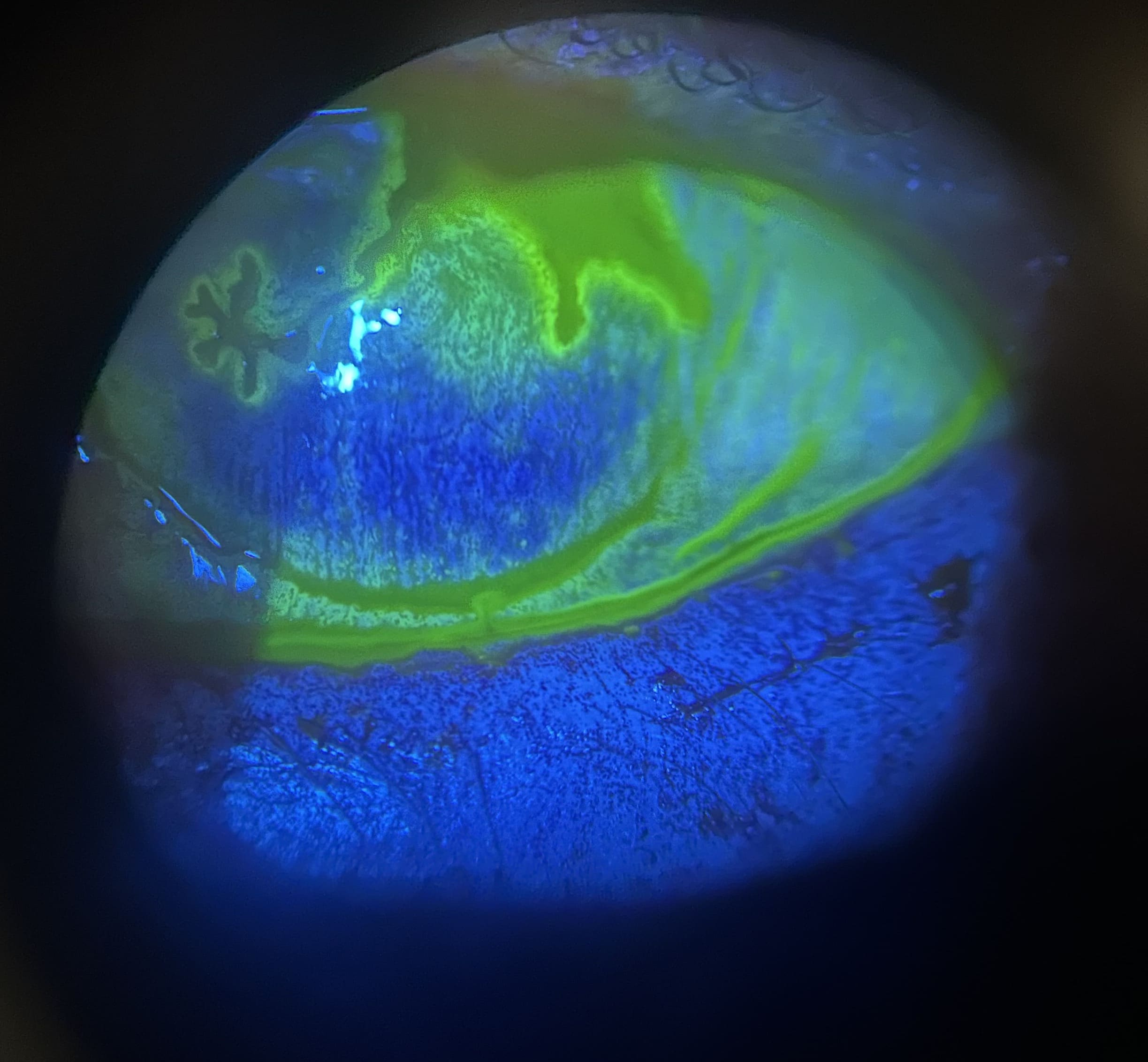
The slit lamp shows a dendritic ulcer — classically this a thin, linear, branching epithelial ulceration with club-shaped terminal bulbs at the end of each branch.
Excellent demonstration of a dendritic ulcer from RootAtlas
Q2. What is the differential diagnosis of this type of lesion?
Answer and interpretation
- HSV keratitis
- Acanthamoeba keratitis pseudodendrites
- Herpes zoster
- Recurrent corneal erosion (may be dendritiform if healing)
- Vaccinia keratitis (classically a complication of smallpox vaccination)
Q3. What should be assessed on history?
Answer and interpretation
History:
- Painful red eye, altered vision, foreign body sensation, photophobia, tearing; usually unilateral
- Skin (e.g., eyelid) vesicular rash may be present
- History of previous episodes of HSV (nasal, oral or ocular)
- Triggers? — may include fever, stress, trauma, immunosuppression or recent topical or steroid use, and ultraviolet light exposure
- History of contact lens use? (acanthamoebae may mimic HSV)
Q4. What features should be assessed on examination?
Answer and interpretation
Examination:
- Visual acuity — may be reduced due to a central corneal ulcer or tearing.
- External examination: Skin — clear vesicles on an erythematous base that progress to crusting. They heal without scarring and cross dermatomes (usually localised to the eyelids when present, and be present bilateral). Corneal sensation — may be decreased (check before applying topical anesthesia)
Slit lamp examination
- Conjunctiva: acute unilateral follicular conjunctivitis +/- conjunctival dendrites +/- geographic ulcers.
- Cornea: dendritic keratitis — edges stain with rose bengal, central ulcer stains with fluorescein.
- Multiple other types lesions may occur:
- geographic ulcers — a large, amoeba-shaped corneal ulcer with a dendritic edge), ghost ulcers (subepithelial scar)neurotrophic ulcers — associated with stromal melting and perforationdisciform keratitis — stromal edema with an intact epitheliumnecrotizing interstitial keratitis — multiple or diffuse, whitish corneal stromal infiltrates with or without an epithelial defect
Primary herpes simplex virus (HSV) infection is usually not apparent clinically, but may be present (especially in children) and may be devastating in neonates (e.g. CNS and multi-organ involvement)
Q5. What is the appropriate investigation and management?
Answer and interpretation
The diagnosis is usually made clinically — although scrapings/ swabs of lesions may be used for confimation by viral culture.
Ophthalmology referral for assessment the next day.
Antiviral therapy:
- Start treatment with topical antivirals.
- consider topical aciclovir ointment 5 times daily for skin lesions (unproven)
- Trifluridine 1% drops (e.g., Viroptic) nine times per day or vidarabine 3% ointment (e.g., Vira-A) five times per day for conjunctival or corneal epithelial involvement
If corneal stromal disease or complications are present an ophthalmologist may initiate treatment with topical steroids and/ or systemic antivirals. Sometimes corneal debridement is required.
Other treatment
- Oral analgesia
- warm or cool soaks to skin lesions tds
- cycloplegics for AC involvement or photophobia
- treat complications
Q6. What are the possible complications of this condition?
Answer and interpretation
- corneal scarring, melting or perforation
- uveitis and hypopyon
- retinitis
- glaucoma
- permanent visual loss
- bacterial and fungal superinfection
- permanent visual loss
Q7. What should be suspected if the lesion fails to resolve over 2-3 weeks?
Answer and interpretation
- noncompliance
- topical antiviral toxicity (discontinue topical antivirals)
- neurotrophic ulcer
- Acanthamoeba keratitis (perform smears)
References
- Ehlers JP, Shah CP, Fenton GL, Hoskins EN. The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease Lippincott Williams & Wilkins
- NSW Statewide Opthalmology Service. Eye Emergency Manual — An illustrated Guide. [Free PDF]
- Mahmood AR, Narang AT. Diagnosis and management of the acute red eye. Emerg Med Clin North Am. 2008 Feb;26(1):35-55, vi. PMID: 18249256.

OPHTHALMOLOGY BEFUDDLER
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
