
![]()
Eponymyth: The Moseley Stitch-Up™
While today’s genuine clinical updates include the AHA/ACC dropping a new A-to-E severity classification for acute pulmonary embolisms, we felt it was equally important to address a far more insidious emergency department crisis.
Every clinician knows the profound frustration of the ultrasound-guided foreign body removal. You locate the shard of glass or rogue splinter on the US monitor, make your incision, and then… the object playfully darts around the subcutaneous tissues like a greased pig on ice.
You might try searching for a quick fix using the newly launched FOAM Cortex AI clinical search tool, but even advanced AI cannot save you from the physical reality of an evasive foreign body. Traditionalists suggest “patience” or “better lighting.”
Enter The Moseley Stitch-Up™ — a groundbreaking technique designed to end this game of subcutaneous Tom & Jerry.
🥸 EPONYMYTHOLOGY
We frequently use the LITFL platform to revere pioneers of the craft and the Moseley Stitch-Up™ absolutely belongs in this pantheon of aggressive problem-solving. First described (and subsequently denied) by Dr Chris Moseley during a particularly challenging clinical shift — one in which he grew tired of chasing a sewing needle around a bricklayer’s heel — this technique flips the script on foreign body removal.
After all, if Rogozov could scoop out his own appendix in a frozen Antarctic hut using a handheld mirror and pure spite, you can certainly lasso a wayward palm frond with a loop of Prolene and a dream. When asked about the honour, Dr Moseley reportedly stated: “I didn’t agree to this.”
The Clinical Problem: “The Slip-and-Slide”
Foreign bodies in the soft tissue are not stationary objects; they are nomadic entities. Every time you apply pressure with a scalpel or forceps, the laws of physics — specifically the “Greased Pig” principle — dictate that the object shall retreat further into the abyss.
You know the one. You see it beautifully on ultrasound… you advance confidently… and suddenly it’s gone. A subtle shift. A betrayal. A game of soft-tissue hide and seek. A lesson anyone who has watched a colleague confidently say “I can see it right there” before spending 2 hours chasing a splinter through multiversal layers of subcutaneous fat will appreciate deeply.
As Rippey eloquently describes in Ultrasound Case 053 — a beautifully frustrating case of sea urchin spines in the plantar surface of a foot — the echogenicity, size, direction of penetration, and patient cooperation vary greatly, presenting the clinician with a considerable challenge. Rippey’s sage counsel: if you fail after a couple of attempts, stop — a fresh set of eyes in the controlled setting of an operating theatre will be better. He also reminds us that it is far easier to remove a foreign body after a few days once it becomes encapsulated and surrounded by inflammatory fluid.
Sage advice indeed… but what if you never again had to admit defeat by employing the classic Moseley Stitch-Up™ technique?
Instead of going to the FB, you bring the FB to you.
Moseley Classification of FB Evasion
| Type | Description | Management |
|---|---|---|
| Type I | Visible, cooperative | Standard retrieval |
| Type II | Visible, intermittently evasive | Standard retrieval ± mild frustration |
| Type III | Visible only when you’re not holding the probe | The Moseley Stitch-Up™ |
| Type IV | “I literally just saw it” | The Double Moseley |
| Type V | Spiritual presence only | Best managed expectantly |
Solution: The Moseley Stitch-Up™
One technique to rule them all, one transducer to find them,
Moslocrates
one suture to bring them up, and in the subcutis bind them.
☝KEY CONCEPT
The principle is elegant in its audacity. When a foreign body proves elusive under ultrasound guidance — dancing away from your forceps with the insouciance of a thing that knows it’s winning — a deep suture is placed directly beneath it, biting wide through the subcutaneous tissue. As the suture is cinched taut, it cradles the object upward toward the skin surface, simultaneously immobilising it in a subcutaneous noose, promoting it to a position from which removal becomes trivial.
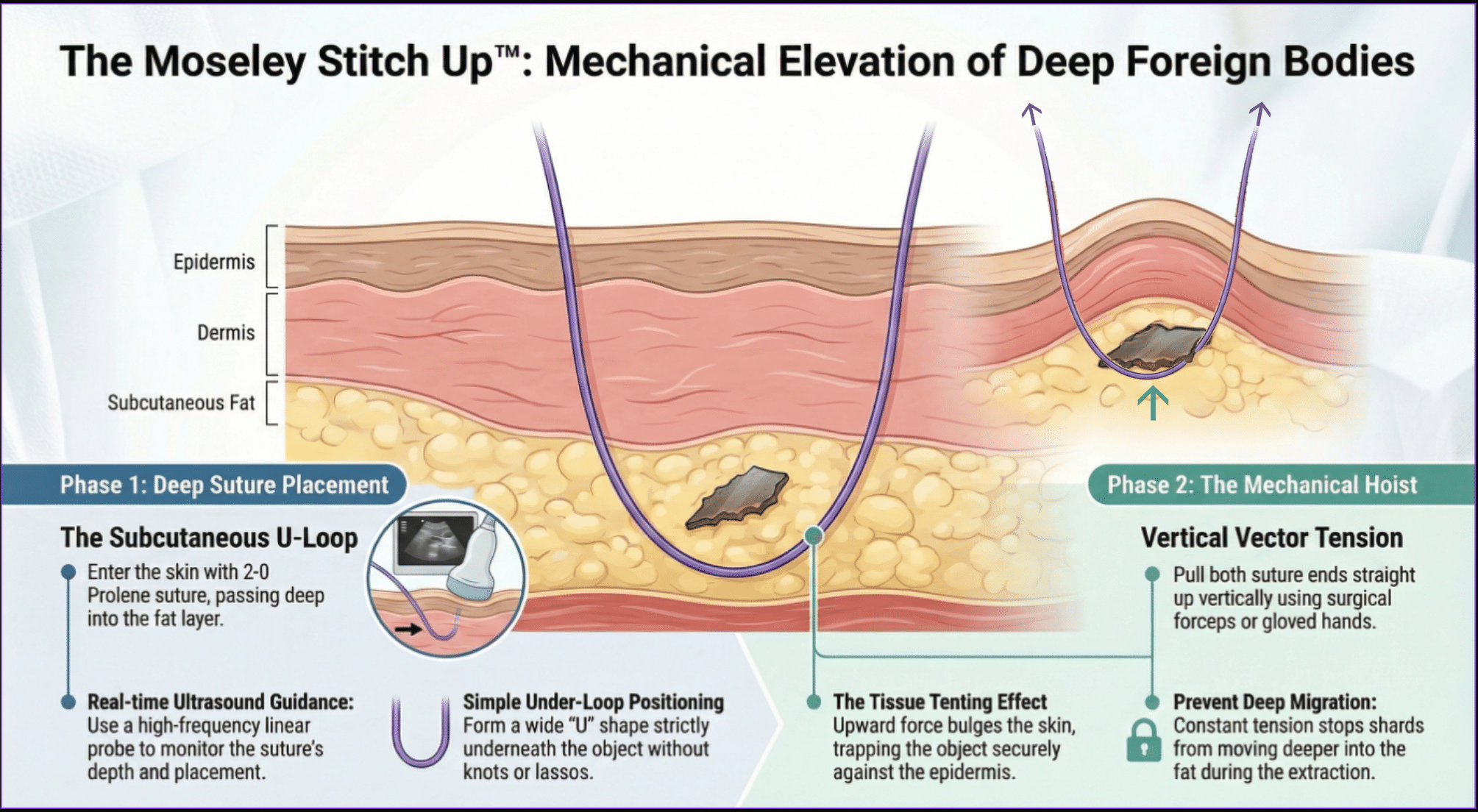
Phase 1. The Subcutaneous U-Loop: — curved needle with 2-0 Prolene passed deep to the FB under real-time ultrasound guidance.
Phase 2. The Mechanical Hoist: vertical vector tension creates a tissue tenting effect, trapping the FB against the epidermis and preventing deep migration during extraction.
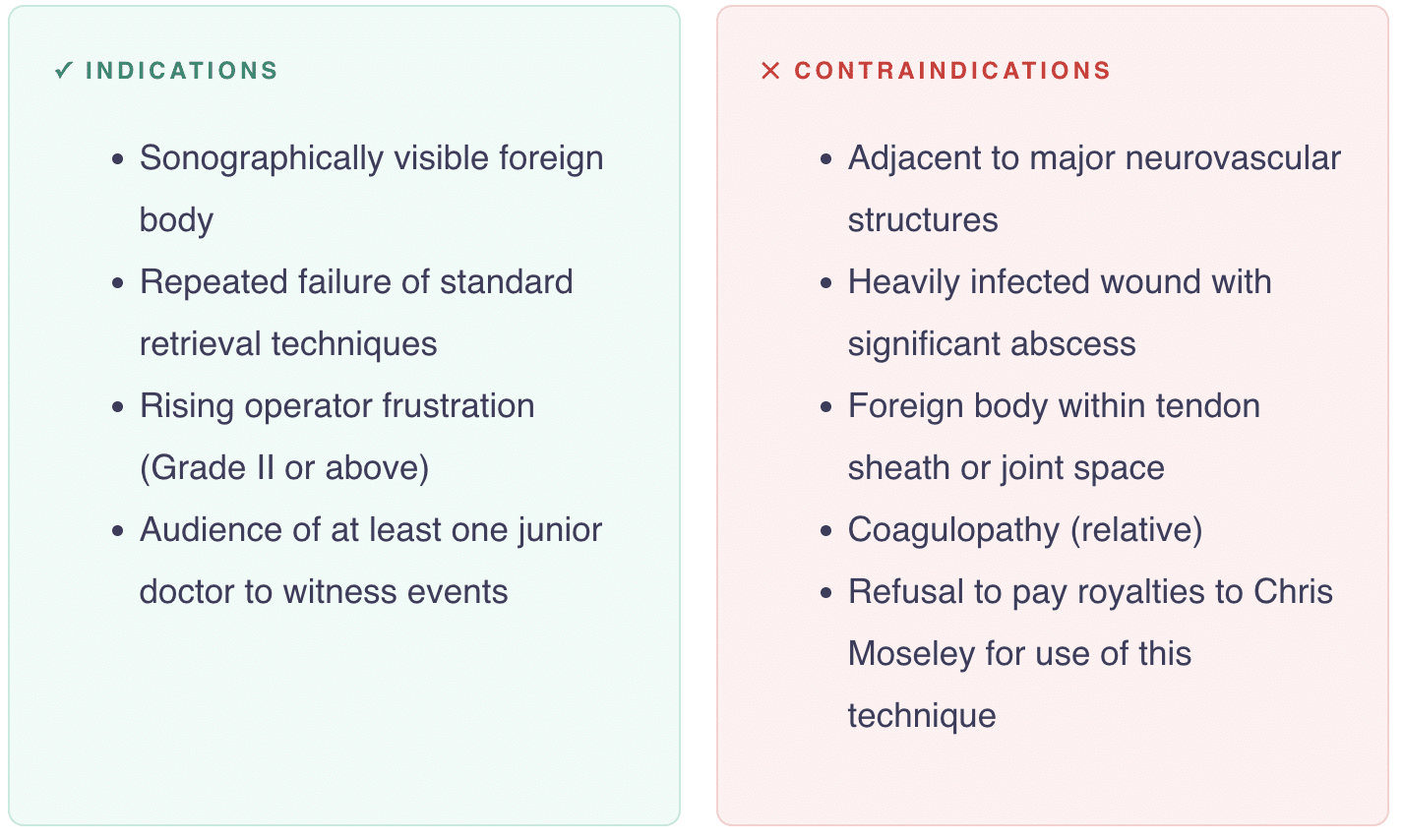
Indications & Contraindications
Equipment

Technique: Step-by-Step
1. Sonographic Surveillance
Identify the FB under ultrasound. Achieve optimal visualisation in two planes.
Verbally confirm: “There it is.”
Keep the probe static. Do not blink.
2. Anaesthetise
Use a regional anaesthetic technique wherever possible — ankle blocks for the sole of the foot, peripheral nerve blocks for the palm. Avoid injecting local anaesthetic directly onto the foreign body — the hydrostatic pressure may displace it further. Instead, use this as an opportunity to show off to everyone around you by employing an ultrasound-guided regional anaesthetic technique. Be sure to announce multiple times to the room what type of complicated nerve block you are performing — before, during and after infiltration. Preferably a novel technique no one has heard of that sounds like an Urban Dictionary entry.
3. Attempt Standard Retrieval
Fail at least twice to establish procedural legitimacy.
4. Reconfirm Position
Note that the foreign body has moved approximately 3–7 mm, as is tradition. This is the way…
5. Deploy Moseley Stitch-Up™ aka “Big Bite”
Using a large-bore non-absorbable suture on a curved cutting needle (Prolene, or literal fishing line if that’s all you’ve got), enter the skin approximately 1 cm lateral to the object under real-time out-of-plane ultrasound guidance. Take a decisive, full-thickness bite of tissue, directing the curved needle deep — well underneath the ultrasound-identified FB. Execute a profound, sweeping arc that encompasses the tissue bed holding the intruder. Exit the skin on the opposite side. You have now lassoed the foreign body.
6. Cinch and Immobilise — “The Elevation”
Grab both ends of the suture and pull upward with the confidence of a Victorian-era strongman. As you tension the suture, the FB is compressed against the underside of the dermis. It is now trapped, immobilised, and physically hoisted toward your blade. The foreign body has been psychologically and physically subdued.
Confirm stabilisation on ultrasound. It has been Moseleyed.
🤩 TOP TIP
For Type IV evasion, consider placing two parallel stabilisation sutures — one on each side of the planned extraction point — creating a corral that prevents lateral escape. The Double Moseley. Chris would be twice as honoured, we’re sure.
Fine print: double royalties apply for double glory.
7. Proceed to Retrieval — “The Pinch”
While an assistant maintains upward traction, make a small incision directly over the FB using a No. 11 blade. Under continuous ultrasound guidance, advance alligator forceps to grasp the FB. Now that the foreign body has been stitched up — held firmly against the skin in its subcutaneous hammock — it cannot escape and is easily removed intact. Confirm complete removal on ultrasound: scan in two planes. Cut and remove the stabilisation suture. Irrigate. Close or leave open per clinical judgement and level of indemnity.
Why It is “Superior”
| Feature | Standard Retrieval | The Moseley Stitch-Up™ |
|---|---|---|
| Search Time | 45 mins – 3 hours | 30 seconds |
| Incision Size | “Keyhole” (initially) | Minimal (unless you slip) |
| Success Rate | Variable | 100%* |
| Patient Satisfaction | Low (bloody mess) | High (impressed by the “hoist”) |
| Eponymous Glory | None | Moseley-grade |
| Teachable Moment | “Maybe try again?” | “Sometimes you just have to commit” |
* Or you’ve caught a nerve. See Complications.
Pearls & Pitfalls
✅ ADVANTAGES
- Eliminates foreign body migration
- Restores operator dominance
- Highly satisfying tactile feedback
- Use the transverse view for suture placement — best cross-sectional view of the needle passing deep to the FB
- Switch to longitudinal view for extraction — best view of forceps approaching the long axis
- Works best with FBs 0.5–3 cm in length in loose subcutaneous tissue
- A curved needle is essential — the arc naturally sweeps deep to the FB and back up to the skin surface
- Can be combined with the “Clothesline” marker needle technique for additional landmarking
- Remember Rippey’s pearl from Case 053: if the Stitch-Up™ isn’t appropriate, delayed removal after a few days allows encapsulation
Complications (The Fine Print)
While the Moseley Stitch-Up™ is revolutionary, some “experts” (naysayers) suggest that “taking a massive blind bite of deep tissue” might occasionally involve unintended structures.
❌ PITFALLS
- The “Double Catch”: Occasionally, you may stitch the foreign body to the local neurovascular bundle. This makes the final removal… spicy. (US guidance mitigates this — this is not, despite the tone, a blind procedure.)
- The Garrotte Effect: If pulled too hard, the FB may simply be bifurcated. You now have two foreign bodies. Double the fun!
- Senior clinician appearing silently over your shoulder mid-cinch
- Do not use on significantly degraded organic FBs — compression may cause fragmentation
- Always scan in two orthogonal planes after removal — residual fragments are easily missed
Operator Experience
Initial hesitation followed by disproportionate confidence. Brief moment of triumph. Followed by reflective questioning of life choices.
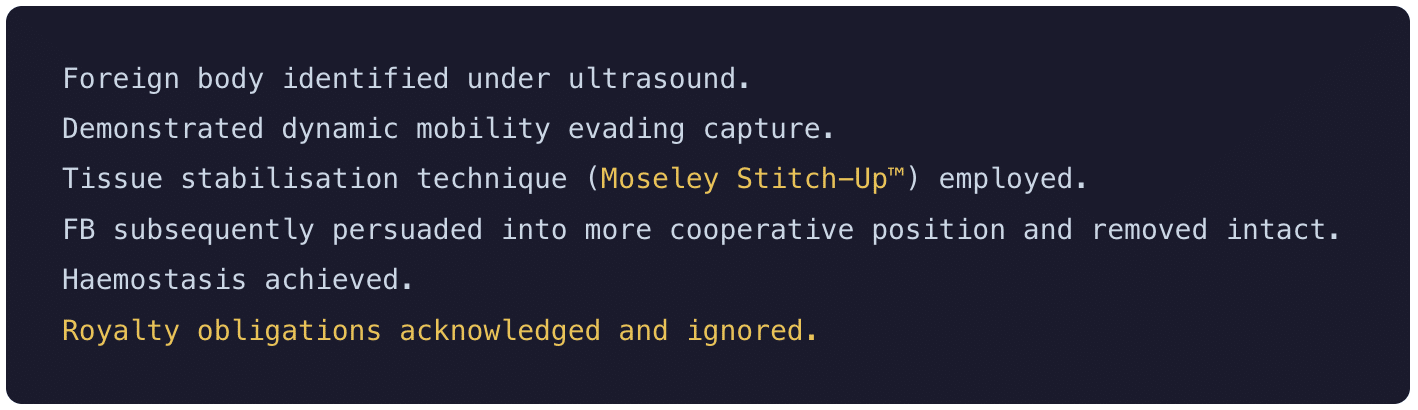
Documentation Example
Consent, Billing & Documentation
Consent
Verbal consent recommended. Suggested phrasing: “We may need to use an advanced technique if it keeps moving.” Avoid elaboration unless directly asked.
Billing & Coding
No current MBS item number, though proposals exist under: “Complex foreign body retrieval with emotional escalation.” Time-based billing may apply (includes time spent explaining the technique to colleagues afterwards).
Conflict of Interest
Authors declare a complex financial relationship with Life in the Fast Lane, including theoretical royalty streams, emotional investment, and a vague intention to invoice someone at some point. No payments have been received to date, though several have been discussed enthusiastically. Ongoing royalty obligations to Chris Moseley for use of the technique remain currently unenforced, but ethically binding. Funds may contribute to keeping the site ad-free in perpetuity, or be redirected towards a misplaced house deposit.
Documentation Example
Follow-Up Advice
Review in 48 hours or sooner if: pain increases, swelling increases, patient Googles the procedure, or patient asks what “stitch-up” means.
Teaching Pearls
🙌 PEARLS
“See one, do one, immediately regret one”
“The key is confidence, not accuracy”
“If you can see it, you can stitch around it”
“Sometimes you just have to commit”
Historical Context & Evidence Base
There is no randomised controlled trial evidence for this specific technique — there rarely is for novel procedural innovations in emergency medicine, and even more rarely for techniques named after colleagues on April 1st.
The technique is based on sound mechanical principles — physically preventing displacement of a mobile object during extraction — and draws on existing evidence supporting ultrasound-guided foreign body removal (sensitivity 90–98%), percutaneous stabilisation techniques used in orthopaedic and interventional radiology, and suture-based tissue manipulation in dermatological surgery.
Further research is needed, though not actively encouraged.
Summary
| What | Temporary percutaneous suture placed deep to a mobile subcutaneous FB — hoisting it towards the skin surface in a subcutaneous lasso |
| Why | Eliminates FB migration and restores operator dominance |
| When | Moseley Classification Type III–IV evasion; particularly at 3am |
| How | Curved needle + Prolene passed under US deep to FB → cinch taut → FB hoisted against dermis → extract with alligator forceps |
| Key Pearl | The suture acts as a subcutaneous hammock — denying the FB its right to freedom of movement |
| Evidence | Level V (expert opinion under duress) |
| Eponym | Created by Dr Chris Moseley, Stitch-Up specialist |
References
- Rippey J. Ultrasound Case 053 — Sea urchin spines, plantar surface of foot. LITFL POCUS Self-Assessment Quiz. LITFL
- Lyon M, Brannam L, Johnson D, Blaivas M, Duggal S. Detection of soft tissue foreign bodies in the presence of soft tissue gas. J Ultrasound Med. 2004 May;23(5):677-81
- Moseley C, et al. (2026). The Classic Stitch-Up. Journal of Undisputedly Unpublished Emergency Medicine. Level V evidence (expert opinion under duress). External validation pending.
- Moseley C. Personal communication. “I didn’t agree to this.” 2026.
This April 1st, stop chasing and start hoisting.
The Moseley Stitch-Up™ isn’t just a procedure — it’s a power move.
While conventional techniques remain first-line, the Moseley Stitch-Up™ represents an important addition to the emergency physician’s cognitive toolbox — particularly at 3am.
The best April Fools’ posts contain a kernel of genuine clinical utility.
This one contains an entire technique. You’re welcome!
UCEM Core Content
- Utopian College of Emergency for Medicine (UCEM)
- UCEM Publications and Position Statements
- UCEM Mission Statement and Essential Roles and Core Competencies
- About the Utopian College. Including Education; Examinations; and Collegial Hierarchy
- Utopian Medicine General News

MBBS Bsc DPMSA Msc(PH) FACEM FRCEM CCPU. Emergency physician & DDU Fellow, Sir Charles Gairdner Hospital. Favourite colour: hot pink. Favourite food: brussels sprouts. Often found lost in the dynamic range, elbow deep in a gel bath, knobologising for focal clarity