
![]()
The power of social media leads to reversal
Christopher Watford contacted the LITFL team with a query regarding a Visual Aid Question (VAQ) from the first sitting of the 2007 examination ACEM examination. We set about investigating the query using the power of social media…
For me, this scenario has been fascinating for a number of reasons:
- I have observed first hand the power of social media in medical education. The LITFL team were be able to readily and rapidly access a large number of eminent emergency physicians, cardiologists and electrophysiologists and receive timely and accurate responses.
- This fellowship examination case involves an ECG that has been seen by countless examiners, examinees and registrars in training…yet it has taken many years before one astute reader has posted a comment that led us to review, interrogate and question the appropriateness of the scenario ECG
- Is there fear and trepidation surrounding public comment? The fact is that I am sure others have made a similar observation when reviewing this question yet failed to alert us of the issues. Was this lack of feedback associated with emergency physicians being too time-poor, too indecisive or too catatonically apathetic to comment?
- Finally I wonder if the abnormality was actually picked up by the candidates and examiners during the examination marking process but deemed too insignificant to warrant comment in the official examiners report…?
Anyway… Enough hyperbole —here is the VAQ question replicated in full from the first sitting of the fellowship written examinations form 2007 — can you spot the issue?
ACEM Examination Scenario:
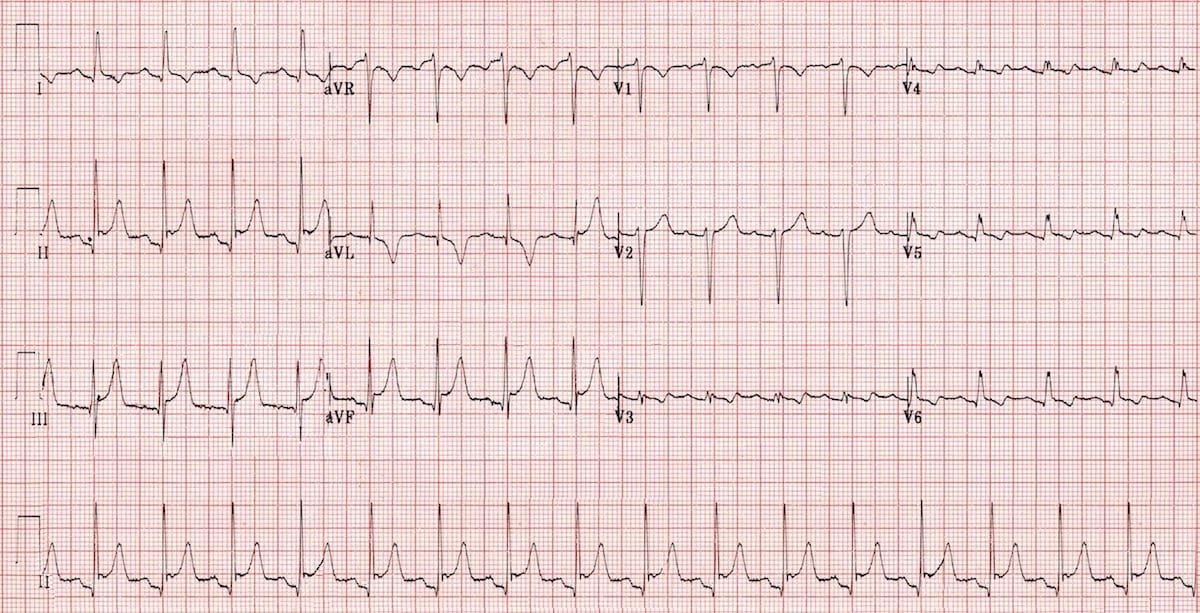
A 49 year old woman presents to your emergency department with central chest pain. BP 110/70, sO2 97% RA:

Q. Describe and interpret her ECG
ACEM Answer and Interpretation
- Overall pass rate for this question was 32/55 (58.2%).
- ECG showed widespread T wave inversion, concave up ST elevation and PR depression inviting in this clinical context a discussion re a number of differentials including pericarditis.
- This was viewed as a difficult but relevant ECG which was satisfactorily interpreted by most candidates.
- The discussion re echocardiography was generally superficial and was the major reason for poor scores.
The #FOAMed discussion
The pertinent observer
It appears that the ECG has a limb lead mixup…I’m having trouble conceiving of pericarditis with the T-waves so deeply inverted in III/aVF.
I believe the following lead configuration may have been used (with the limb leads on the body): – RA: Green – LA: White – RL: Red – LL: Black
It would preserve P-waves in II and aVF and invert T’s in II/III/aVF. Leads I/aVR/aVL would remain relatively undisturbed. Does that seem feasible?
The Cardiologist
Sure looks like it could be LA/LL limb lead reversal. The large P wave and QRS voltage in I and smaller QRS voltage in aVF makes this quite likely (II becomes I and aVF becomes aVL).
Usual QRS axis in a normal EKG is about 60, but LA/LL limb lead reversal is commonly missed because P wave axis and QRS axis still fall within normal range when it occurs.
I must say, the PR segment depression in I (actually II) and elevation in R, paired with the lower precordial voltage makes pericarditis an likely culprit, IMO (along with a waywardly-trained nurse). 🙂
The Electrophysiologist
Hey, nice ECG and nice example of LL reversal. It is definitely left leg – left arm (LA/LL) reversal. Lead I is II and II is I and III is upside down as expected.
Overall – looks like pericarditis to me. ST depression in aVR is most specific for this. Reconstructing the ECG there is significant St elevation in inferior leads.
I would echo just to check inferior wall moving as ST elevation greatest there, and no effusion (lateral complexes look small).
Mark Perrin MD
The Reversal
The KISS principle
- Left Arm and Left Leg Lead reversal…
- Lead I is actually lead II → Lead II is actually lead I and Lead III is inverted
- aVR is normal; AVL is actually aVF and aVF is actually aVL

- RA—right arm; LA—left arm; LL—left leg;
- Clockwise rotation: RA→LA→LL→RA;
- Anti-clockwise rotation: RA→LL→LA→RA.
- The (-) sign signifies that the respective lead is inverted
Chris Nickson…gives us lowly ER docs some take home basics!
References
- ECG Limb lead reversal – ECG Library
- Left arm/right arm lead reversal – ECG Library
- Batchvarov VN, Malik M, Camm AJ. Incorrect electrode cable connection during electrocardiographic recording. Europace. 2007 Nov;9(11):1081-90. PMID 17932025
ECG LIBRARY
Electrocardiogram
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |
