
![]()
ECG Limb Lead Reversal
Accidental misplacement of the limb lead electrodes is a common cause of ECG abnormality and may simulate pathology such as ectopic atrial rhythm, chamber enlargement or myocardial ischaemia and infarction
When the limb electrodes (LA, RA, LL) are exchanged without disturbing the neutral electrode (RL/N), Einthoven’s triangle is “flipped” 180 degrees or rotated, resulting in leads that switch positions, become inverted or remain unchanged (depending on their initial position and vector).
Exchanging one of the limb electrodes with the neutral electrode (RL/N) disrupts Einthoven’s triangle and distorts the zero signal received from Wilson’s central terminal, altering the appearance of both limb and precordial leads. Limb leads may be grossly affected, taking on the appearance of other leads or being reduced to a flat line.
Definitions
Electrodes
- LA = left arm
- RA = right arm
- LL = left leg
- RL/N = right leg (neutral electrode)
Leads
- Bipolar leads: I, II, III
- Augmented unipolar leads: aVL, aVF, aVR
- Wilson’s central terminus (WCT): the ‘zero’ lead, produced by averaging signals from the limb electrodes
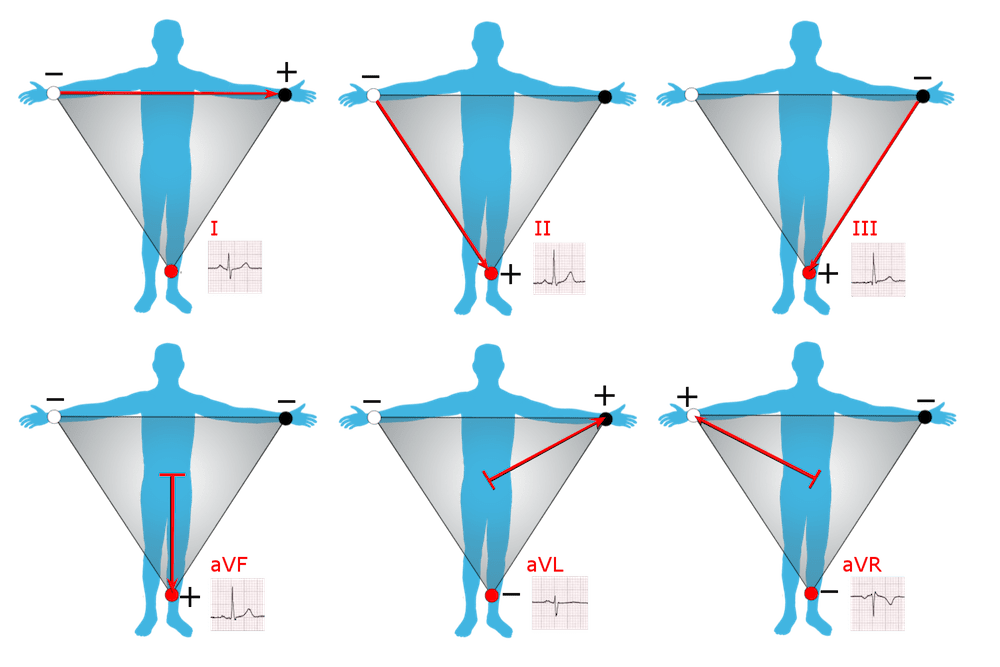
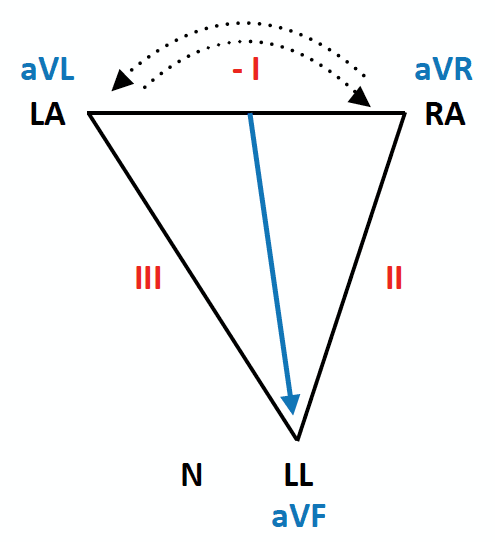
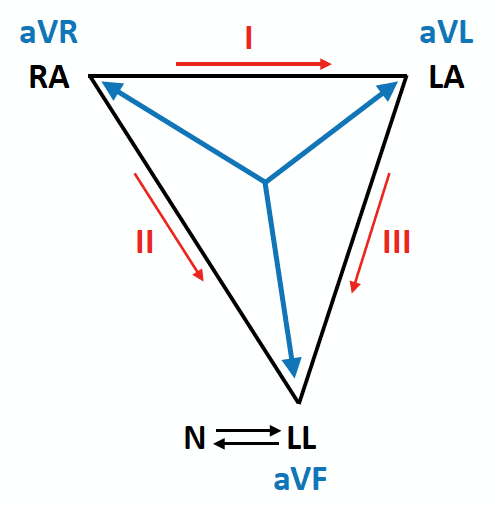
Einthoven Triangle
The relationship between the limb leads and electrodes is described by Einthoven triangle.

Each lead has a specific quantity and direction (vector) produced by adding or subtracting voltages from the recording electrodes.
Bipolar leads
- Lead I is the voltage difference between the LA and RA electrodes (LA – RA), directed towards LA at zero degrees.
- Lead II is the voltage difference between the LL and RA electrodes (LL – RA), directed towards LL at +60 degrees.
- Lead III is the voltage difference between the LL and LA electrodes (LL – LA), directed towards LL at +120 degrees.
Augmented Unipolar leads
- Lead aVL is directed towards the LA electrode (-30 degrees), calculated as follows: aVL = LA – (RA + LL)/2.
- Lead aVF is directed towards the LL electrode (+90 degrees), calculated as follows: aVF = LL – (LA + RA)/2.
- Lead aVR is directed towards the RA electrode (-150 degrees), calculated as follows: aVR = RA – (LA + LL)/2.
Wilson’s central terminus
- This directionless “zero lead” lead is calculated as the average input from the three limb leads: WCT = 1/3 (RA + LA + LL).
An understanding of Einthoven’s triangle and the mathematical derivations of each lead will help us in understanding the ECG patterns produced by each type of limb lead reversal.
LA/RA reversal
With reversal of the LA and RA electrodes, Einthoven’s triangle flips 180 degrees horizontally around an axis formed by lead aVF.
This has the following effects on the ECG:
- Lead I becomes inverted
- Leads II and III switch places
- Leads aVL and aVR switch places
- Lead aVF remains unchanged
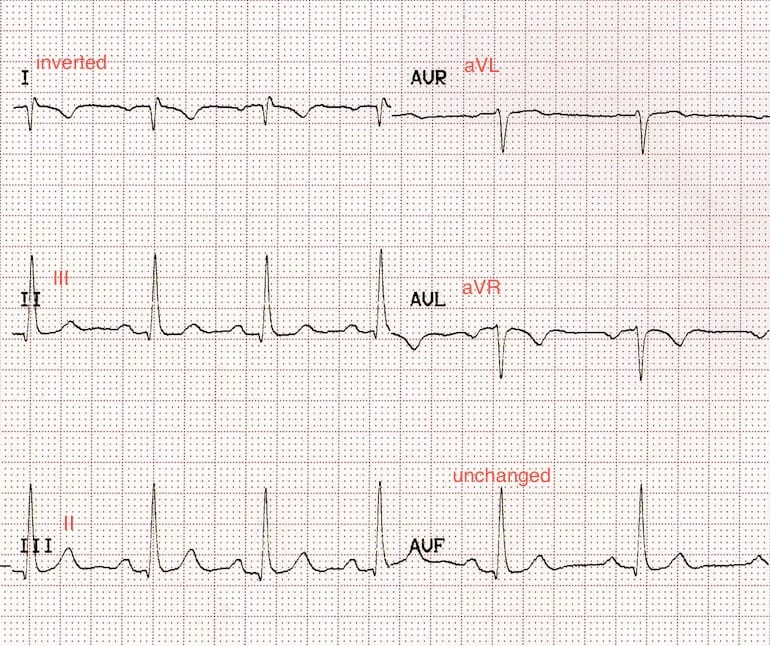

Quick guide to spotting LA/RA reversal
- Lead I is completely inverted (P wave, QRS complex and T wave)
- Lead aVR often becomes positive
- There may be marked right axis deviation
LA/RA reversal may simulate dextrocardia. However, in contrast to dextrocardia there is normal R wave progression in the precordial leads.

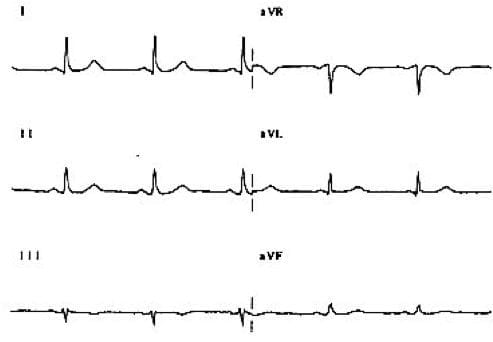
LA/LL reversal
With reversal of the LA and LL electrodes, Einthoven’s triangle rotates 180 degrees vertically around an axis formed by aVR.
This has the following effects on the ECG:
- Lead III becomes inverted
- Leads I and II switch places
- Leads aVL and aVF switch places
- Lead aVR remains unchanged

Quick guide to spotting LA/LL reversal
- Lead III is completely inverted (P wave, QRS complex and T wave)
- The P-wave is unexpectedly larger in lead I than lead II (it is usually the other way around)
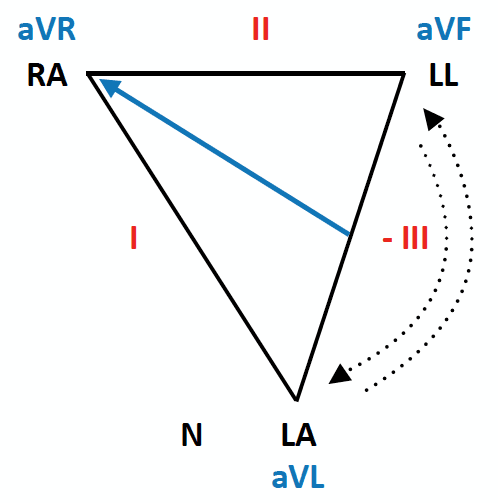
RA/LL reversal
With reversal of the RA and LL electrodes, Einthoven’s triangle rotates 180 degrees vertically around an axis formed by aVL.
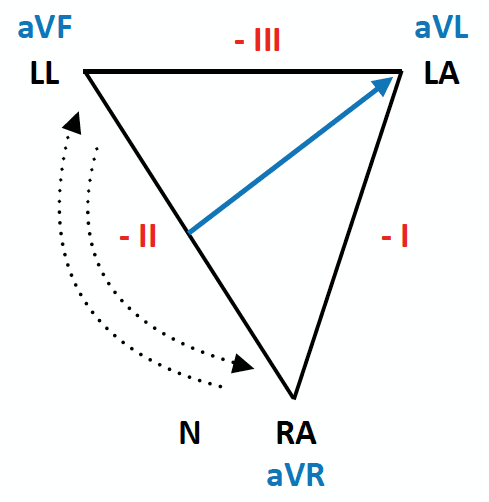
This has the following effects on the ECG:
- Lead II becomes inverted
- Leads I and III become inverted and switch places
- Leads aVR and aVF switch places
- Lead aVL is unchanged
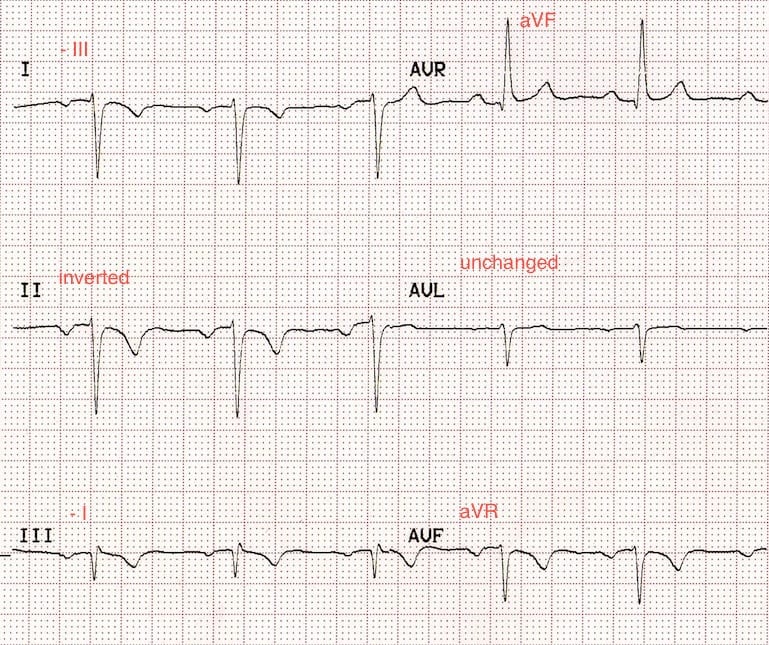
Quick guide to spotting RA/LL reversal
- Leads I, II, III and aVF are all completely inverted (P wave, QRS complex and T wave)
- Lead aVR is upright
RA/RL(N) reversal
With reversal of the RA and RL(N) electrodes, Einthoven’s triangle collapses to very thin “slice” with the LA electrode at its apex.
- The RA and LL electrodes now record almost identical voltages, making the difference between them negligible (i.e, lead II = zero)
- Lead aVL runs within this thin slice, facing approximately opposite to lead III
- Displacement of the neutral electrode renders leads aVR and aVF mathematically identical, such that they appear exactly alike (but different to the baseline ECG)
RA/RL(N) lead reversal has the following ECG features:
- Lead I becomes an inverted lead III
- Lead II records a flat line (zero potential)
- Lead III is unchanged
- Lead aVL approximates an inverted lead III
- Leads aVR and aVF become identical
As the neutral electrode has been moved, the precordial voltages may also be distorted.

Quick guide to spotting RA/RL(N) reversal
- Lead II is a flat line
LA/RL(N) reversal
With reversal of the LA and RL(N) electrodes, Einthoven’s triangle collapses to very thin “slice” with the RA electrode at its apex.
- The LA and LL electrodes now record almost identical voltages, making the difference between them negligible (i.e. lead III = zero).
- Lead aVR runs within this thin slice, facing approximately opposite to lead II.
- The displacement of the neutral electrode renders leads aVL and aVF mathematically identical, such that they appear exactly alike (but different to the baseline ECG).
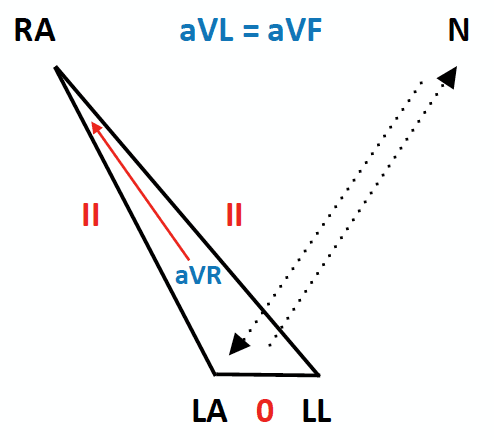
LA/RL(N) lead reversal has the following ECG features:
- Lead I becomes identical to lead II
- Lead II is unchanged
- Lead III records a flat line (zero potential)
- Lead aVR approximates to an inverted lead II
- Leads aVL and aVF become identical
As the neutral electrode has been moved, the precordial voltages may also be distorted.
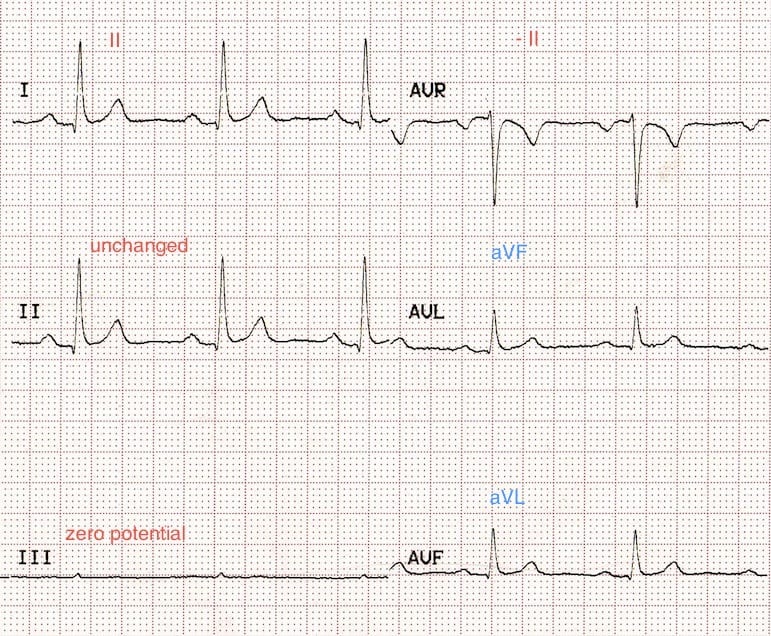
Quick guide to spotting LA/RL(N) reversal
- Lead III is a flat line
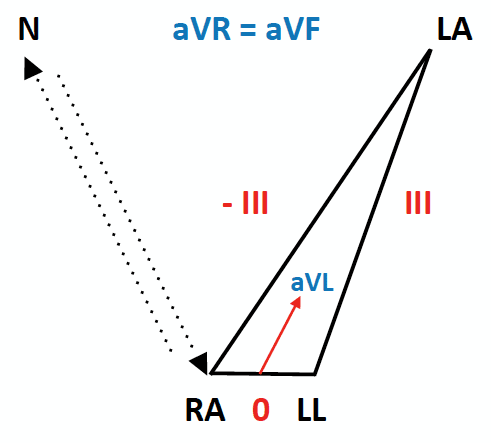
Bilateral Arm-Leg Reversal (LA-LL plus RA-RL)
If the electrodes on each arm are swopped with their corresponding leg electrode (LA with LL, RA with RL), Einthoven’s triangle collapses to a very thin slice with the LL electrode at its apex.
- The RA and LA electrodes (now sitting on adjacent feet) record almost identical voltages, which makes the difference between them negligible (i.e. lead I = zero)
- Leads II, III and aVF all become identical (equivalent to inverted lead III), as they are all now measuring the voltage difference between the left arm and the legs
- The displacement of the neutral electrode renders leads aVL and aVR mathematically identical, such that they appear exactly alike (but different to the baseline ECG)

Bilateral arm-leg reversal has the following ECG features:
- Lead I records a flat line (zero potential)
- Lead II approximates an inverted lead III
- Lead III is inverted
- aVR and aVL become identical
- aVF looks like negative lead III
As the neutral electrode has been moved, the precordial voltages may also be distorted.

Quick Guide To Spotting Bilateral Arm-Leg Reversal
- Lead I is a flat line
LL/RL(N) reversal
- With reversal of the lower limb electrodes, Einthoven’s triangle is preserved as the electrical signals from each leg are virtually identical.
- The ECG is therefore unchanged.
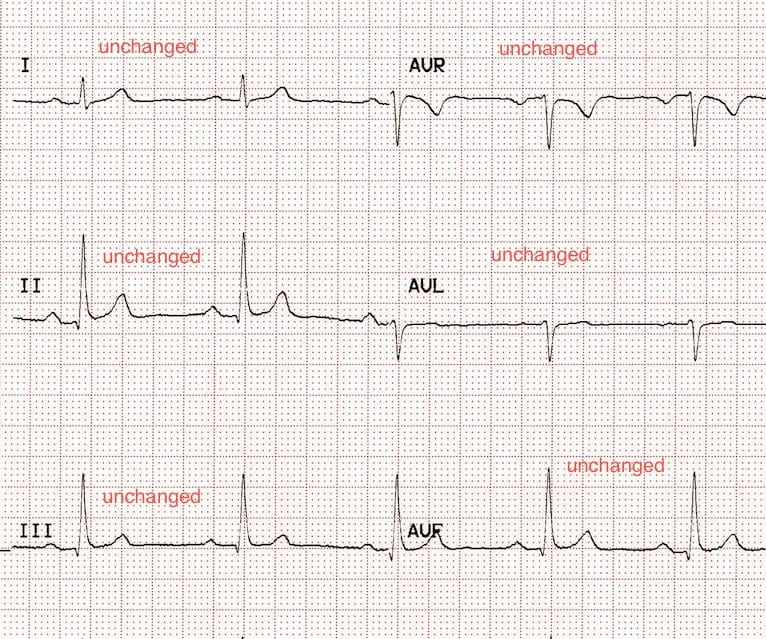
How to spot LL/RL(N) reversal
- You won’t!
But don’t worry, it won’t make any difference to your ECG interpretation.
Summary – The KISS Principle

- RA—right arm; LA—left arm; LL—left leg;
- Clockwise rotation: RA→LA→LL→RA;
- Anti-clockwise rotation: RA→LL→LA→RA.
- The (-) sign signifies that the respective lead is inverted
References
- ECG Top 100 – ECG Case 078
- The power of social media leads to reversal – LITFL
- Batchvarov VN, Malik M, Camm AJ. Incorrect electrode cable connection during electrocardiographic recording. Europace. 2007 Nov;9(11):1081-90. PMID 17932025
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.
Thank you, very concise and easy to understand!
Very helpful!