
![]()
Translational Simulation
OVERVIEW
Translational simulation aims to directly improve patient care and healthcare systems, through diagnosing safety and performance issues and delivering simulation-based interventions (Brazil, 2017).
- It is a functional descriptor of simulation in that the focus is on the purpose of the simulation activities, irrespective of the location, modality, or content
- Translational simulation seeks to drive organizational learning by targeting simulation at the systems level as well as its components, whereas traditional simulation-based education primarily addresses learning by individuals or small groups.
GUIDING PRINCIPLES
Successful translational simulation is guided by the following principles (Nickson et al, 2021):
- A systems approach (recognises the complexity of factors that contribute to a problem, and that may provide a solution; this leads to a greater likelihood of meaningful and sustained impact)
- Stakeholder involvement (right stakeholders at the right time) leading to participatory design and co-creation
- Forms a strategy, not an event (it is an iterative process)
- Disciplined focus to address a defined problem (though this focus may shift or evolve iteratively)
- Functional task alignment (simulation activities chosen are aligned with the desired objectives to achieved the desired outcomes)
Translational simulation may be performed as small scale in house projects led by frontline clinicians with relevant skills (e.g. departmental guideline for a procedure or work process) or may be a large scale project led by dedicated staff (e.g. clinical space design and testing during construction of a new healthcare facility). Regardless of the scope and scale, the guiding principles still apply.
DIAGNOSTICS, INTERVENTIONS, AND HEALTHCARE PERFORMANCE
Primary uses of translational simulation (Nickson et al, 2021) are to:
- improve quality through targeted interventions focused on clinical performance and/or patient outcomes
- design and test planned infrastructure or interventions
- explore work environments and/or people in them
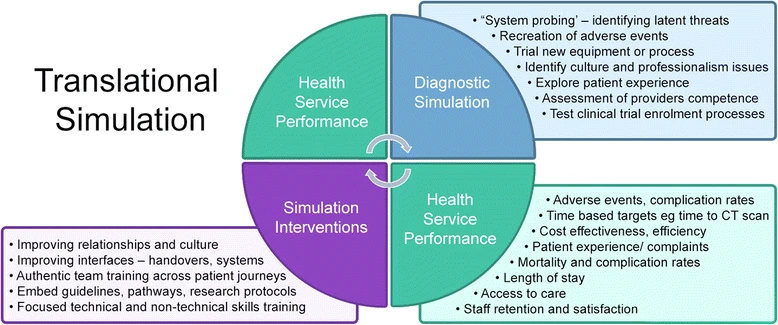
Figure 1, from Brazil (2017), shows the inter-relation of healthcare performance targets and the simulation strategies that may be used.
- Healthcare performance targets may be be used to indicate problems to address or be used to measure the outcomes of translation simulation strategies.
- Translation simulation may involve diagnostic simulations used to identify problems and the simulation interventions that may be used to address them.
OPERATIONAL APPROACH TO TRANSLATIONAL SIMULATION
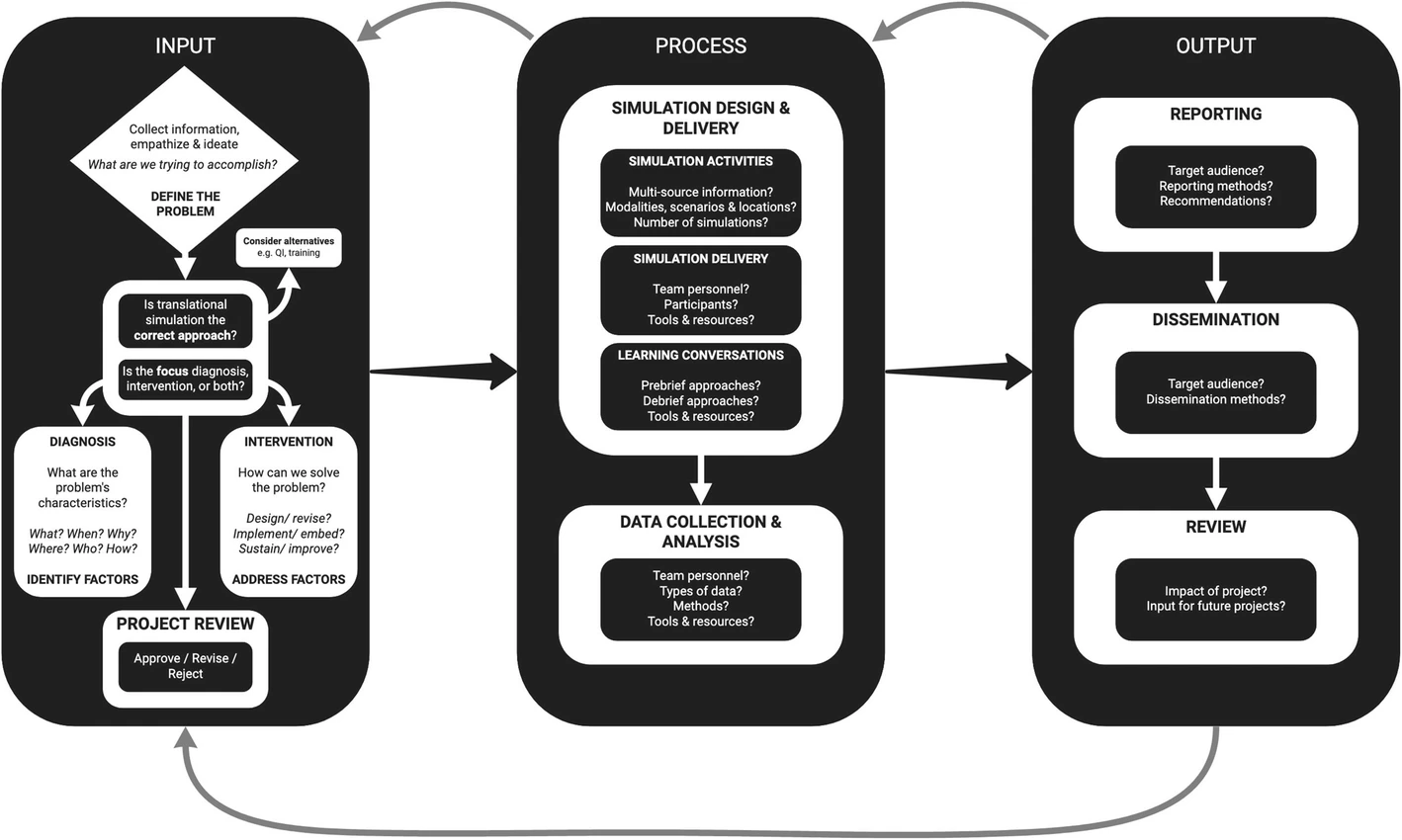
The input-process-output framework of translational simulation (see Figure 2) provides a model for how translational simulation projects can be undertaken. Note that although the phases are described in a linear fashion, the process is iterative with frequent revisiting and revision of previous phases as the project develops. The phases, and important considerations at each step, are discussed in detail in Translational Simulation: from description to action by Nickson et al (2021).
Input phase (see Table 1 of Nickson et al (2021) for further considerations)
- Define the problem
- Answer the question “what are we trying to accomplish?” by collecting information, empathising with frontline workers involved, and ideating
- Is translational simulation the correct approach?
- Determine whether translational simulation is an appropriate strategy to address the problem, or whether it should be used in combination with other strategies
- Determine if the initial focus should be diagnostic, interventional, or both
- Diagnosis – seeks to identify factors that contribute to the problem
- Intervention – seeks to address these contributing factors to solve the problem
- Project review
- Consider whether approve, revise, or reject the project proposal based on the above
Process phase (see Table 2 of Nickson et al (2021) for further considerations)
- Simulation delivery and design
- Identification and design of appropriate simulation activities based on multi-source information, with consideration of the optimal number of simulation activities to perform and appropriate use of modalities, scenarios, and locations.
- Delivery of simulation involving carefully chosen delivery team personnel as well as participants, aided by appropriate tools and resources (e.g. simulation equipment, checklists, etc)
- Conduct learning conversations with attention to approaches to prebrief and debrief of simulation activities, and the use of tools and resources (e.g. debriefing frameworks, AV support, etc)
- Data collection and analysis
- Consideration of the team required, types of data to be collected (quantitiative and/or qualitative), methods used, and tools and resources required (e.g. validated observation tools, AV recording equipment, etc)
Output phase (see Table 3 of Nickson et al (2021) for further considerations)
- Reporting findings and key recommendations using appropriate methods tailored to the target audience (e.g. Hospital leadership versus frontline workers involved in simulations)
- Dissemination of appropriate findings to a wider target audience (e.g. hospital employees, journal publication, etc) using appropriate methods
- Review of the impact of the translational simulation project and implications for future projects
PUBLISHED EXAMPLES AND EVIDENCE
The articles cited below provide examples and published evidence for the benefit of translational simulation. Many also include tips and tools that are useful for developing translational simulation strategies.
Translational simulation strategies have been used to:
- Improve patient outcomes
- More-active in situ mock code participation (17/100 beds/year) was associated with higher in hospital cardiac arrest survival (odds ratio = 0.62; 95% CI: 0.54-0.72) than less-active participation (3/1– beds/year) in a multi-center study (Josey et al, 2018). Previously, the number of paediatric mock codes performed was shown to correlate with improved in-hospital cardiac arrest survival (Andreatta et al, 2011).
- Improve the performance and quality of patient care
- Decreased door-to-needle times for stroke thromboprophylaxis (Ajmi et al, 2019)
- Improved trauma patient care including: decreased time to blood transfusion adminstration for trauma patients (Gray et al, 2021), decreased time spent in trauma bay by trauma patients prior to transfer to CT (Knobel et al, 2018), and improved trauma team teamwork and task completion scores (Steinemann et al, 2011).
- Improved pediatric emergency airway management process measures (Long et al, 2017) and compliance with the NEAR4KIDS quality improvement bundle for airway management (Colman et al, 2021)
- Develop and redesign patient care team structures, processes and procedures
- identify latent design threats, prototype design solutions, and help orientate staff to new teams, processes and procedures.
- Examples include medical emergency team responses (Wheeler et al, 2013), emergency departments (Patterson et al, 2013), ECPR (Extracorporeal life support cardiopulmonary resuscitation) guidelines (Ross et al, 2019) and latent safety threats (Stoner et al, 2022), and readiness for opening of new hospitals (Kaba and Barnes, 2019), including paediatric services (Geis et al, 2011) and obstetric services (Ventre et al, 2014).
- Perform clinical systems testing and aid the design of built environments for patient care
- identify latent system design threats, prototype design solutions, and help orientate staff to new clinical spaces
- Approaches include the use of healthcare failure modes and effects analysis (HFMEA) (Nielsen et al, 2014; Barlow et al, 2017; Colman et al, 2019a; Colman et al, 2019b), the use of the SAFEE debriefing tool (Colman et al, 2020), and Design Thinking-Informed simulation (Petrosoniak et al, 2020).
- Promote culture change and improve relationships
- Qualitative studies show that translational simulation impacts on hospital culture and helps improve relationships, including aspects such as the development of shared goals, shared knowledge, communication and mutual respect (Brazil et al, 2019; Purdy et al, 2020)
- Rapidly adapt and transform health services and processes for pandemic preparedness
- numerous examples during the COVID19 pandemic including departments such as maternity services (Lowe et al, 2020), hospital-wide approaches (Brazil et al, 2020; Brydges et al, 2020; Dieckmann et al, 2020; Li et al, 2020), and even health system-wide approaches (Dubé et al; 2020).
CHALLENGES AND FUTURE DIRECTIONS
Translational simulation is still maturing, in terms of the concept itself and approaches used. Future directions and challenges, some of which are discussed in more detail in Nickson et al (2021), include:
- Demonstrating return on investment (ROI) and how to balance potential benefits with resource costs
- Further integration of translational simulation strategies with other quality improvement and human factors/ ergonomics approaches
- Building capacity for translational simulation within healthcare
- Response to the COVID pandemic and adaptation to the post-pandemic world
- Ensuring safety and avoiding unintended consequences of translational simulation (Raemer et al, 2018; Jafri et al, 2022; Brazil et al, 2022)
- Understanding and awareness of the limitations of work-as-simulated as a proxy for work-as-done (Shorrock, 2022).
CONCLUSION
Translational simulation can improve patient care and health systems performance.
- An input-process-output model can be used for the delivery of translational simulation by adhering to key guiding principles
- Research into translational simulation, and how to achieve optimal outcomes through its delivery, is still in its infancy
VIDEO SLIDECAST
[cite]
References and Links
FOAM and web resources
- Bond Translational Simulation Collaborative
- Hospital News – Translational simulation connects learnings to patient outcomes
- Humanistic Systems – Proxies for Work-as-Done: 6. Work-as-Simulated
- Simulcast – 124 Advances in Simulation: Translational Simulation in Action (podcast)
Journal articles
- Ajmi SC, Advani R, Fjetland L, et al. Reducing door-to-needle times in stroke thrombolysis to 13 min through protocol revision and simulation training: a quality improvement project in a Norwegian stroke centre. BMJ Qual Saf. 2019;28(11):939-948. doi:10.1136/bmjqs-2018-009117 [article]
- Andreatta P, Saxton E, Thompson M, Annich G. Simulation-based mock codes significantly correlate with improved pediatric patient cardiopulmonary arrest survival rates. Pediatr Crit Care Med. 2011;12(1):33-38. doi:10.1097/PCC.0b013e3181e89270 [pubmed]
- Barlow M, Dickie R, Morse C, Bonney D, Simon R. Documentation framework for healthcare simulation quality improvement activities. Adv Simul (Lond). 2017;2:19. Published 2017 Oct 17. doi:10.1186/s41077-017-0053-2 [article]
- Brazil V. Translational simulation: not ‘where?’ but ‘why?’ A functional view of in situ simulation. Adv Simul (Lond). 2017;2:20. Published 2017 Oct 19. doi:10.1186/s41077-017-0052-3 [article]
- Brazil V, Purdy E, Alexander C, Matulich J. Improving the relational aspects of trauma care through translational simulation. Adv Simul (Lond). 2019;4:10. Published 2019 May 21. doi:10.1186/s41077-019-0100-2 [article]
- Brazil V, Lowe B, Ryan L, et al. Translational simulation for rapid transformation of health services, using the example of the COVID-19 pandemic preparation. Adv Simul (Lond). 2020;5:9. Published 2020 Jun 3. doi:10.1186/s41077-020-00127-z [article]
- Brazil V, Scott C, Matulich J, Shanahan B. Developing a simulation safety policy for translational simulation programs in healthcare. Adv Simul (Lond). 2022;7(1):4. Published 2022 Jan 24. doi:10.1186/s41077-022-00200-9 [article]
- Brydges R, Campbell DM, Beavers L, et al. Lessons learned in preparing for and responding to the early stages of the COVID-19 pandemic: one simulation’s program experience adapting to the new normal. Adv Simul (Lond). 2020;5:8. Published 2020 Jun 3. doi:10.1186/s41077-020-00128-y [article]
- Colman N, Doughty C, Arnold J, et al. Simulation-based clinical systems testing for healthcare spaces: from intake through implementation. Adv Simul (Lond). 2019;4:19. Published 2019 Aug 2. doi:10.1186/s41077-019-0108-7 [article]
- Colman N, Stone K, Arnold J, et al. Prevent Safety Threats in New Construction through Integration of Simulation and FMEA. Pediatr Qual Saf. 2019;4(4):e189. Published 2019 Jun 24. doi:10.1097/pq9.0000000000000189 [article]
- Colman N, Dalpiaz A, Walter S, Chambers MS, Hebbar KB. SAFEE: A Debriefing Tool to Identify Latent Conditions in Simulation-based Hospital Design Testing. Adv Simul (Lond). 2020;5:14. Published 2020 Jul 28. doi:10.1186/s41077-020-00132-2 [article]
- Colman N, Newman JW, Nishisaki A, Register M, Gillespie SE, Hebbar KB. Translational Simulation Improves Compliance with the NEAR4KIDS Airway Safety Bundle in a Single-center PICU. Pediatr Qual Saf. 2021;6(3):e409. Published 2021 May 19. doi:10.1097/pq9.0000000000000409 [article]
- Dieckmann P, Torgeirsen K, Qvindesland SA, Thomas L, Bushell V, Langli Ersdal H. The use of simulation to prepare and improve responses to infectious disease outbreaks like COVID-19: practical tips and resources from Norway, Denmark, and the UK. Adv Simul (Lond). 2020;5:3. Published 2020 Apr 16. doi:10.1186/s41077-020-00121-5 [article]
- Dubé M, Kaba A, Cronin T, Barnes S, Fuselli T, Grant V. COVID-19 pandemic preparation: using simulation for systems-based learning to prepare the largest healthcare workforce and system in Canada. Adv Simul (Lond). 2020;5:22. Published 2020 Aug 18. doi:10.1186/s41077-020-00138-w [article]
- Geis GL, Pio B, Pendergrass TL, Moyer MR, Patterson MD. Simulation to assess the safety of new healthcare teams and new facilities. Simul Healthc. 2011;6(3):125-133. doi:10.1097/SIH.0b013e31820dff30 [pubmed]
- Gray A, Chartier LB, Pavenski K, McGowan M, Lebovic G, Petrosoniak A. The clock is ticking: using in situ simulation to improve time to blood administration for bleeding trauma patients. CJEM. 2021;23(1):54-62. doi:10.1007/s43678-020-00011-9 [article]
- Jafri FN, Shah S, Yang CJ, et al. Safety Considerations for In Situ Simulation in Closed SARS-CoV-2 Units. Simul Healthc. 2022;17(1):49-53. doi:10.1097/SIH.0000000000000542 [pubmed]
- Josey K, Smith ML, Kayani AS, et al. Hospitals with more-active participation in conducting standardized in-situ mock codes have improved survival after in-hospital cardiopulmonary arrest. Resuscitation. 2018;133:47-52. doi:10.1016/j.resuscitation.2018.09.020 [pubmed]
- Kaba A, Barnes S. Commissioning simulations to test new healthcare facilities: a proactive and innovative approach to healthcare system safety. Adv Simul (Lond). 2019;4:17. Published 2019 Jul 16. doi:10.1186/s41077-019-0107-8 [article]
- Knobel A, Overheu D, Gruessing M, Juergensen I, Struewer J. Regular, in-situ, team-based training in trauma resuscitation with video debriefing enhances confidence and clinical efficiency. BMC Med Educ. 2018;18(1):127. Published 2018 Jun 7. doi:10.1186/s12909-018-1243-x [article]
- Li L, Lin M, Wang X, Bao P, Li Y. Preparing and responding to 2019 novel coronavirus with simulation and technology-enhanced learning for healthcare professionals: challenges and opportunities in China. BMJ Simul Technol Enhanc Learn. 2020;6(4):196-198. doi:10.1136/bmjstel-2020-000609 [article]
- Long E, Cincotta DR, Grindlay J, et al. A quality improvement initiative to increase the safety of pediatric emergency airway management. Paediatr Anaesth. 2017;27(12):1271-1277. doi:10.1111/pan.13275 [pubmed]
- Lowe B, De Araujo V, Haughton H, Schweitzer J, Brazil V. Preparing maternity for COVID-19: A translational simulation approach. Aust N Z J Obstet Gynaecol. 2020;60(4):628-632. doi:10.1111/ajo.13185 [article]
- Nickson CP, Petrosoniak A, Barwick S, Brazil V. Translational simulation: from description to action. Adv Simul (Lond). 2021;6(1):6. Published 2021 Mar 4. doi:10.1186/s41077-021-00160-6 [article]
- Nielsen DS, Dieckmann P, Mohr M, Mitchell AU, Østergaard D. Augmenting health care failure modes and effects analysis with simulation. Simul Healthc. 2014;9(1):48-55. doi:10.1097/SIH.0b013e3182a3defd [pubmed]
- Patterson MD, Geis GL, Falcone RA, LeMaster T, Wears RL. In situ simulation: detection of safety threats and teamwork training in a high risk emergency department. BMJ Qual Saf. 2013;22(6):468-477. doi:10.1136/bmjqs-2012-000942 [pubmed]
- Petrosoniak A, Hicks C, Barratt L, et al. Design Thinking-Informed Simulation: An Innovative Framework to Test, Evaluate, and Modify New Clinical Infrastructure. Simul Healthc. 2020;15(3):205-213. doi:10.1097/SIH.0000000000000408 [pubmed]
- Purdy E, McLean D, Alexander C, et al. Doing our work better, together: a relationship-based approach to defining the quality improvement agenda in trauma care. BMJ Open Qual. 2020;9(1):e000749. doi:10.1136/bmjoq-2019-000749 [article]
- Raemer D, Hannenberg A, Mullen A. Simulation safety first: an imperative. Adv Simul. 2018;3(1):25. doi: 10.1186/s41077-018-0084-3. [article]
- Ross P, Nickson C, Sheldrake J, McClure J. Using In-Situ Simulation for Extracorporeal Cardiopulmonary Resuscitation (ECPR) Guideline Development. SSRN. 2019; June 25. doi:/10.2139/ssrn.3409806 [article]
- Shorrock, S. Proxies for Work-as-Done: 6. Work-as-Simulated. Humanistic Systems. 13 January 2022. Available at URL: https://humanisticsystems.com/2022/01/13/proxies-for-work-as-done-6-work-as-simulated/
- Steinemann S, Berg B, Skinner A, et al. In situ, multidisciplinary, simulation-based teamwork training improves early trauma care. J Surg Educ. 2011;68(6):472-477. doi:10.1016/j.jsurg.2011.05.009 [pubmed]
- Stoner AC, Schremmer RD, Miller MA, et al. Simulation-Based System Analysis: Testing Preparedness for Extracorporeal Membrane Oxygenation Cannulation in Pediatric COVID-19 Patients. Pediatr Qual Saf. 2022;7(1):e510. Published 2022 Jan 21. doi:10.1097/pq9.0000000000000510 [article]
- Ventre KM, Barry JS, Davis D, et al. Using in situ simulation to evaluate operational readiness of a children’s hospital-based obstetrics unit. Simul Healthc. 2014;9(2):102-111. doi:10.1097/SIH.0000000000000005 [pubmed]
- Wheeler DS, Geis G, Mack EH, LeMaster T, Patterson MD. High-reliability emergency response teams in the hospital: improving quality and safety using in situ simulation training. BMJ Qual Saf. 2013;22(6):507-514. doi:10.1136/bmjqs-2012-000931 [pubmed]
SMILE 2
Better Healthcare
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
