
![]()
Ultrasound Case 026
Presentation
A 34 year old woman presents with intermittent right upper quadrant pain. It is often worse after eating.
View 2: Gallbladder in long axis
Describe and interpret these scans
IMAGE INTERPRETATION
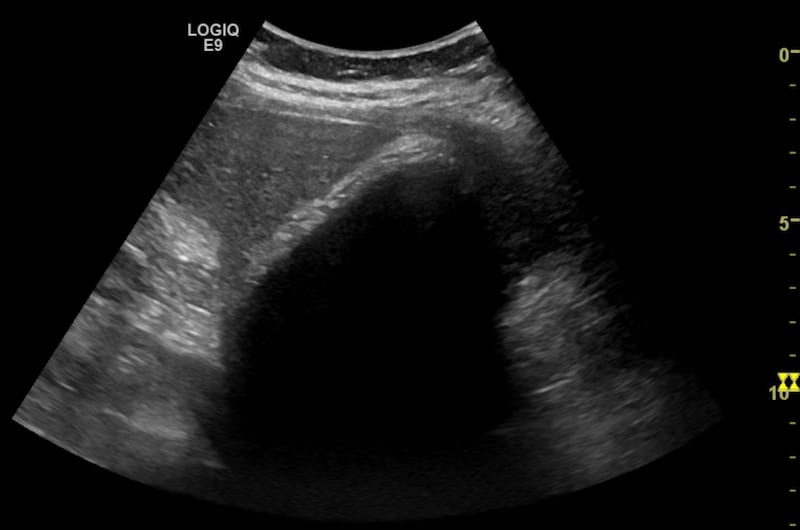
Image 1 & 2: Gallbladder in long axis.
This is a gallbladder completely filled with innumerable small stones.
The homogeneous grey organ in the top left of the image is the liver.
In the centre of the screen is a bright white line running from the gallbladder neck at the lower left to the fundus at the top right. This first white line is the gallbladder wall.
Just deep to this is a thin intermittent hypoechoic line – a trace of bile, and then another line of bright echoes but this time the line is slightly irregular. The echoes are created by numerous gallstones that have filled the gallbladder and are abutting the inner surface of the GB wall.
The gallstones reflect some ultrasound energy but most is absorbed and they cannot be penetrated. This causes a dense dark shadow behind the stones.
These three features, the Wall, Echo and Shadow are known as the WES sign of a GB filled to the brim with tiny stones.
CLINICAL CORRELATION
Wall Echo Shadow sign (WES) of cholelithiasis
The gallbladder is sometimes confused with bowel and vice versa. They can look very similar but there are key features you should look for to ensure you are not making an error.
Is it a gallbladder shaped organ with a fundus and neck, or it it a continuous tubular structure like bowel?
Is there peristalsis?
The Wall: The GB wall is usually echogenic unless it is oedematous. Bowel wall is more often hypoechoic and the traditional layers (serosa, muscularis propria, submucosa, muscularis mucosa, mucosa, lumen) can sometimes be seen.
The Content: May be similar – fluid, debris, gas, or solid material. A common difficulty is confusing gas filled bowel with a stone filled gallbladder. Apart from the shape and peristalsis, look for the signature “WES” where the gallbladder wall is first seen, then a slightly irregular border of many small adjacent stones, and then a very dark acoustic shadow.
Gas in the lumen of bowel tends to cast a brighter / lighter shadow which is often termed a “dirty” shadow. Having said this they can be very hard to differentiate. In the video clip the central dark shadow is cast by WES of many small GB stones. The shadow on the image left is cast by intestinal gas. The initial echo is brighter and the irregularity of the surfaces of the numerous tiny stones not seen, and perhaps the shadow a little more dirty – but in this case it was the position, shape and static nature of the gallbladder that made the operator certain.
[cite]
TOP 100 ULTRASOUND CASES

An Emergency physician based in Perth, Western Australia. Professionally my passion lies in integrating advanced diagnostic and procedural ultrasound into clinical assessment and management of the undifferentiated patient. Sharing hard fought knowledge with innovative educational techniques to ensure knowledge translation and dissemination is my goal. Family, wild coastlines, native forests, and tinkering in the shed fills the rest of my contented time. | SonoCPD | Ultrasound library | Top 100 | @thesonocave |