
![]()
Waxing and Waning Weakness
aka Metabolic Muddle 002
A 50 year old Chinese female presents with severe weakness. She has a history of previous similar episodes that self-resolved.
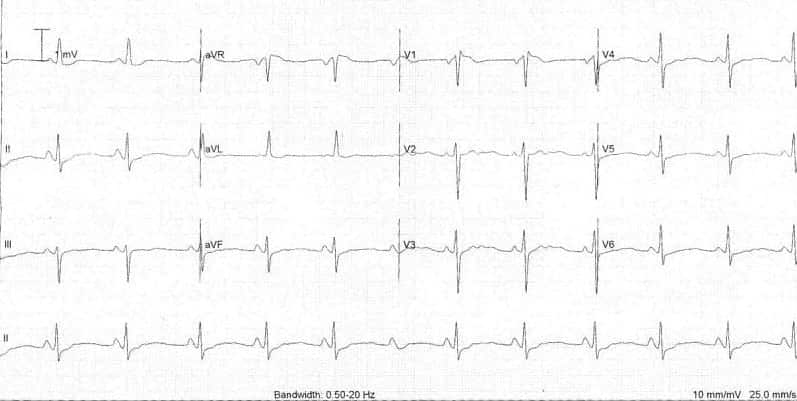
This is her admission ECG:
Questions
Q1. Describe the ECG.
Answer and interpretation
The ECG findings include:
- Sinus rhythm with a rate of 70bpm
- Normal axis
- Flattened T waves with the presence of U waves.
- Normal QTc (Corrected QT)
Q2. What is the likely diagnosis?
Answer and interpretation
Hypokalaemic periodic paralysis
This patient had a potassium of 1.9 mmol/L.
Q3. How is this condition treated?
Answer and interpretation
During an acute attack treatment involves correction of hypokalaemia with potassium supplementation.
For prophylaxis, patients are usually treated with acetazolamide.
Q4. Why is it important to measure the thyroid function?
Answer and interpretation
The major differential here is thyrotoxic periodic paralysis.
Thyrotoxic periodic paralysis also causes periodic paralysis associated with hypokalaemia. Interestingly, the prevalence of thyrotoxic periodic paralysis in patients with thyrotoxicosis is estimated to be 0.1-0.2% in Caucasians and 13-14% in Chinese.
CLINICAL CASES
Metabolic Muddle
Intensivist in Wellington, New Zealand. Started out in ED, but now feels physically ill whenever he steps foot on the front line. Clinical researcher, kite-surfer | @DogICUma |
