
![]()
Wilhelm Lutz
Wilhelm Lutz (1888-1958) was a Swiss dermatologist
Training under notable Dermatologists of the time, namely Josef Jadassohn, Bruno Bloch and Felix Lewandowsky, he eventually became Professor and Head of the Department of Dermatology and Venereology at the University Hospital in Basel, Switzerland.
He is eponymously remembered for first describing several dermatological conditions including Lewandowsky-Lutz syndrome, elastosis perforans serpiginosa and the Lutz sign.
Biography
- Born on November 4, 1888 in Basel
- 1912 – MD, University of Basel
- Trained under Ernst Hedinger (1873-1924) in pathology and Josef Jadassohn (1863-1936) in dermatology; initially assistant at the University Skin Clinic in Basel, then later became Professor (“Oberarzt”).
- Appointed Assistant at University Skin Clinic in Basel by Prof. Bruno Bloch after the completion of his training.
- Spent time training at dermatological clinics under Josef Jadassohn (1863-1936) in Bern and under Bruno Bloch (1973-1933) and Felix Lewandowsky (1879-1921) in Basel.
- 1922 – Associate professor in dermatology following the untimely death of Professor Felix Lewandowsky
- 1937 – Professor and chairman of the newly created chair of dermatology and venereology of the University of Basel.
- Died on September 8, 1958
Medical Eponyms
Lewandowsky-Lutz dysplasia (1922)
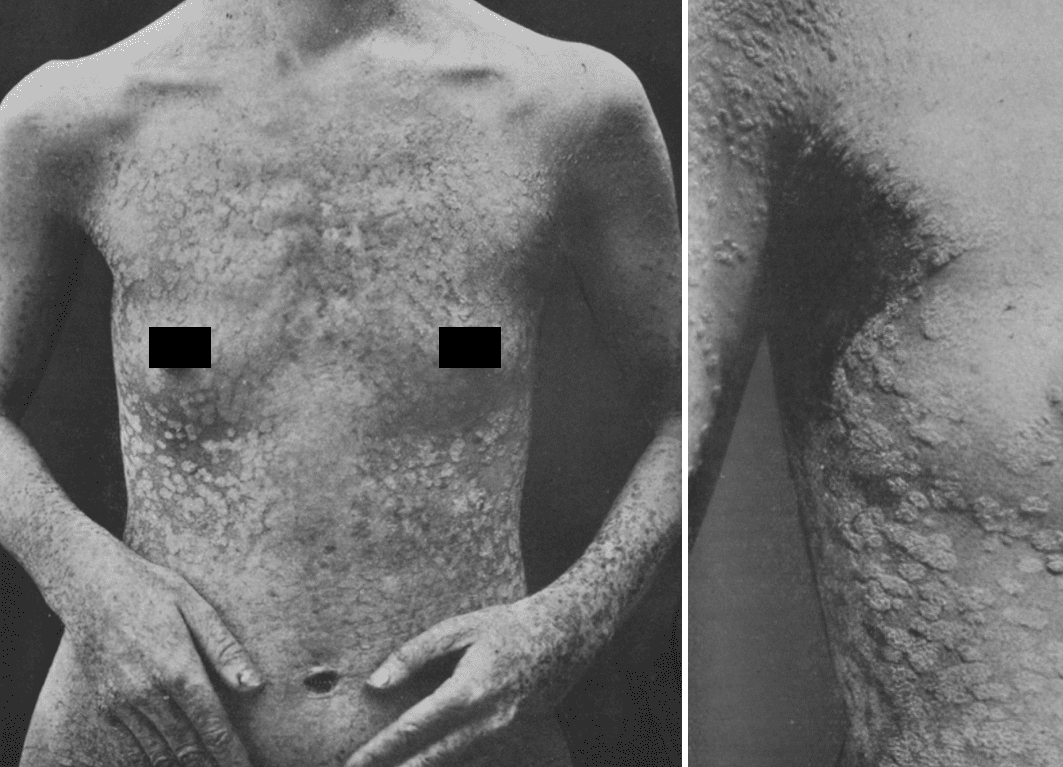
Known as epidermodysplasia verruciformis (EV), Treeman syndrome and Lewandowsky-Lutz syndrome – an extremely rare inherited disorder in which there is widespread and persistent infection with human papilloma virus, a defect in cell-mediated immunity and consequent propensity for malignant transformation.
The disease was first described in 1922 by Lutz and Felix Lewandowsky (1879-1921) and Lutz a condition they called Epidermodysplasia verruciformis.
Lewandowsky and Lutz dysplasia is usually inherited in an autosomal recessive manner. Acquired cases exist (“Acquired epidermodysplasia verruciformis”), which may result from immunocompromise i.e. HIV infection, organ transplantation or cancer.
The disease usually presents in a generalised nature with multiple lesions resembling pityriasis versicolour or thicker lesions resembling seborrheic keratosis. It is associated with a risk of malignant transformation, particularly squamous cell carcinoma or Bowen carcinoma, with sun exposure.
Lutz-Miescher syndrome (elastosis perforans serpiginosa) (1953)
Now known as elastosis perforans serpiginosa, Lutz-Miescher Syndrome is a rare dermatological disorder in which abnormal elastic tissue passes from the dermis to the epidermis, described as transepithelial elimination.
It presents with erythematous keratotic papules (2-5 mm diameter), with small central scaling arranged in linear, serpiginous (snake-like), or circular patterns. These lesions are usually asymptomatic but may be itchy. They most commonly present on the posterior neck (70%), but may also present on the upper limbs, face, legs or trunk.
Elastosis perforans serpiginosa affects males more than females (4:1) and is most common in early adulthood (20-30 years). Its aetiology is not well understood, however likely has a genetic component. It has been categorised into:
- Idiopathic elastosis perforans serpiginosa, possibly genetic
- Reactive elastosis perforans serpiginosa, associated with Ehlers Danlos syndrome, Marfan syndrome and Down syndrome
- Drug-Induced elastosis perforans serpiginosa, affecting 1% of those treated with D-penicillamine
Elastosis perforans serpiginosa has no treatment today, however usually spontaneously resolves after a few years.
Naming History:
Lutz initially described the entity as “Keratosis Follicularis Serpiginosa,” when he described a curious chronic dermatosis in 1953.
Original
English
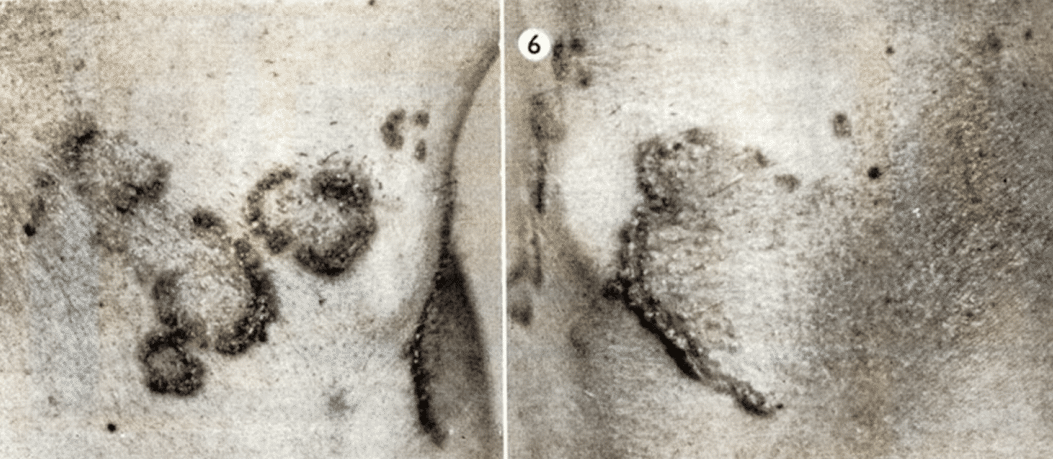
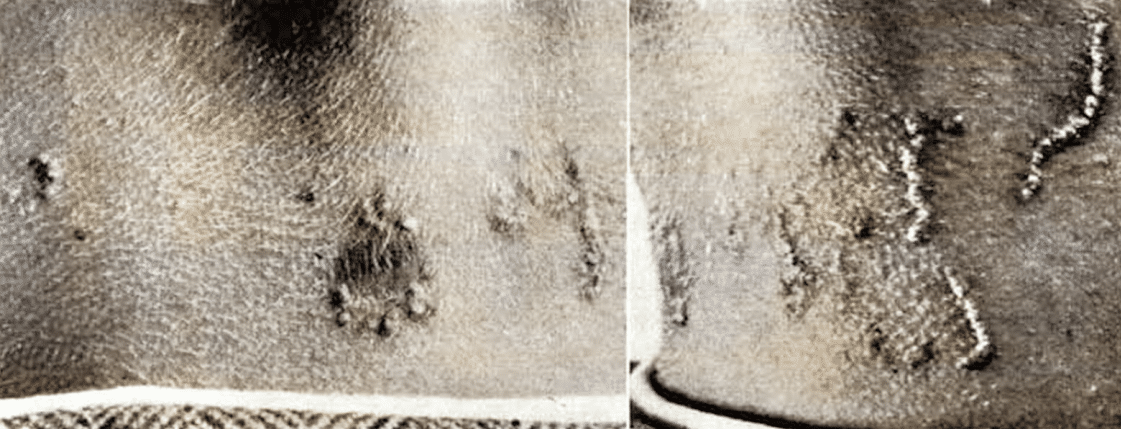
daß sich im Lauf von etwa acht Jahren Herde an beiden Halsseiten entwickelt hätten, die allmählich größer geworden seien, ohne daß er bis jetzt deswegen einen Arzt aufgesucht hätte. An der linken Halsseite findet sich ein größerer, an der rechten finden sieh mehrere kleinere Herde, alle vom selben Aufbau. Sie zeigen einen sehr deutlich ausgeprägten erhabenen serpiginösen leistenartigen peripheren Wall und ein m it einer leichten Atrophie abgeheiltes Zentrum, in dem mehrfach die Follikel noch als kleine Papelchcn hervortreten. Der Randwall besteht aus einzelnen dicht nebeneinander liegenden keratotischen Knötchen. Stellenweise ist der pathologische Prozeß spontan zum Stillstand gekommen, wie dies besonders deutlich an der Begrenzung des breiten an der linken Halsseite weit nach hinten ziehenden geheilten Streifens gut erkennbar ist (Abb. 5 und 6).
…in the course of about eight years, lesions had developed on both sides of the neck, which had gradually increased in size, without him ever having consulted a doctor about them. There is a larger one on the left side of the neck and several smaller ones on the right side, all of the same structure. They show a very clearly pronounced, raised, serpiginous, ridge-like peripheral wall and a center that has healed with a slight atrophy, in which the follicles are still protruding as small papules.
The rim wall consists of individual keratotic nodules lying close together. In places the pathological process has come to a spontaneous standstill, as can be seen particularly clearly from the border of the wide, healed stripe that runs far back on the left side of the neck (Figs. 5 and 6).
Two further clinically identical cases were reported by Ruiter and Beening (1955) and Miescher (1955). Miescher suggested that the condition should be named “elastoma intrapapillare perforans verricuforme” after carefully studying histological changes in the condition. Dammert and Putkonen suggested in 1957 that the condition be named Elastosis Perforans Serpiginosa.
It seems the condition was ultimately referred to as Elastosis Perforans Serpinosa after a 1960 case report by Hashimoto and Hill noted:
“The present lesion has been variously named by several authors. Originally it was named Keratosis Follicularis Serpiginosa by W. Lutz. Subsequently, the terms Elastoma Intrapapillare Perforans Verruciforme and Elastosis Perforans Serpiginosa were suggested by G. Miescher and by Dammert and Putkonen, respectively. As Hitch has pointed out, the elastic tissue increase is not primarily or necessarily “intrapapillar” or “follicular” but in the cutis in general. There is no evidence that it is a tumor, as the suffix “oma” suggests, but a morbid process of abnormal increase in elastic tissue, as the name elastosis might convey. Clinically it takes serpiginous configuration with eruptive individual lesions. Therefore, we feel that the term suggested by Dammert and Putkonen Elastosis Perforans Serpiginosa is more suitable than the others.”
Hashimoto and Hill, 1960
Lutz sign (Asboe-Hansen sign)(1957)
The Lutz sign (otherwise known as the “bulla spread sign”, “Asboe-Hansen sign”, “indirect Nikolsky sign” or “Nikolsky II sign”), refers to the extension of a blister to adjacent unblistered skin when unidirectional pressure is applied to the top of the bulla. This differs from the Nikolsky sign, where slight rubbing of the skin results in exfoliation of the outermost layer, forming a blister within minutes.
In 1957, Lutz described the blister-spread sign in pemphigus vulgaris chronicus
…if one carefully presses upon a blister, it will enlarge within the epidermis in direction of the periphery due to mechanical pressure of the blister fluid in the acantholytic epidermis
…if carefully rubbed on an uninvolved area of skin, the superficial layers of the skin will move and a blister will form after some time (Nikolsky phenomenon).”
Lutz 1957
It was then noted by Asboe-Hansen in 1960 that this phenomenon could be observed in patients with pemphigus vulgaris (acutus), pemphigus foliaceus, pemphigus vegetans, and bullous pemphigoid (pemphigus vulgaris chronicus):
A spreading of blisters can be artificially induced by slight to moderate external finger pressure in pemphigus vulgaris (acutus), pemphigus foliaceus, pemphigus vegetans and bullous pemphigoid (pemphigus vulgaris chronicus). The sign is characteristic, although possibly not absolutely specific, of the pemphigus group of diseases.
It reflects a reduction or loss of intercellular bridges between epidermal cells or a dermal-epidermal lysis. In the new area of the expanded blister, the microscopic picture of a spontaneous fresh blister is reproduced.
Asboe-Hanson 1960
The Lutz sign is elicited by first marking the margin of a blister with a pen, then applying slow and careful unidirectional pressure by a finger to the bulla. This causes the bulla to extend beyond the marked margin.
The Lutz sign is positive in all varieties of blistering diseases such as the pemphigus group of diseases and many cases of subepidermal blisters. A regular rounded border is observed in bullous pemphigoid and other subepidermal blistering disorders. An irregular angulated border is seen in Pemphigus vulgaris, vegetans foliaceus, erythematosus and fogo selvagem and SSSS.
Major Publications
- Lewandowsky F, Lutz W. Ein Fall einer bisher nicht beschriebenen Hauterkrankung (Epidermodysplasia verruciformis). Archiv für Dermatologie und Syphilis, Berlin, 1922; 141: 193-202. [Lewandowsky-Lutz dysplasia]
- Lutƶ W, Siemens HW, Strandberg J. Vererbung Innere Sekretion Stoffwechsel. 1929
- Lutz W. Keratosis follicularis serpiginosa In: III. Présentation de Malades – Krankendemonstrationen. Dermatologica, Basel, 1953; 106: 318-320. [Lutz-Miescher syndrome]
- Lutz W. Pemphigus chronicus vulgaris, In: Lehrbuch der Haut- und Geschlechtskrankheiten. Basel: Karger; 1957: 198-199, 203 [Lutz sign]
References
Biography
- Schuppli R. Prof. Dr. Wilhelm Lutz; 1888-1958. Schweiz Med Wochenschr. 1958 Nov 15;88(46):1165-6.
- Reiss F. Wilhelm Lutz, M.D.; 1888-1958. AMA Arch Derm. 1959 Jun;79(6):724-5.
- Bibliography. Lutz, Wilhelm 1888-1958. WorldCat Identities
Eponymous terms
Lewandowsky-Lutz dysplasia
- Bhutoria B, Shome K, Ghosh S, Bose K, Datta C, Bhattacharya S. Lewandowsky and lutz dysplasia: report of two cases in a family. Indian J Dermatol. 2011 Mar;56(2):190-3.
- Agharbi FZ. Epidermodysplasie verruciforme: à propos d’un cas [Epidermodysplasia verruciformis: about a case]. Pan Afr Med J. 2018;30:78.
- Lee R and Jibreal H. Epidermodysplasia Verruciformis. The Australasian College of Dermatologists, 2020.
Lutz-Miescher syndrome
- Miescher G. Elastoma intrapapillare perforans verruciforme. Dermatologica, Basel, 1955; 110: 254-266.
- Beening, CW and Ruiter, M. Keratosis follicularis serpiginosa. Dermatologica, 110: 175, 1955.
- Dammert, K. AND Putkonen, T. Keratosis follicularis serpiginosa (Lutz). Dermatologiea, 116: 143—155. 1957.
- Hashimoto, K and Hill, W. ELASTOSIS PERFORANS SERPIGINOSA. A CASE REPORT WITH HISTOCHEMICAL AND ENZYME DIGESTION STUDIES. The Journal of Investigative Dermatology, 1960.
Lutz Sign
- Asboe-Hanson, G. Blister-spread induced by finger-pressure, a diagnostic sign in pemphigus. J Invest Dermatol, 1960 Jan;34:5-9.
- Grando, S, et al. History and clinical significance of mechanical symptoms in blistering dermatoses: A reappraisal. Journal of the American Academy of Dermatology, 2003 48(1): 86-92.
- Ganapati, S. Eponymous Dermatological Signs in Bullous Dermatoses. Indian Journal of Dermatology, 2014 Jan-Feb; 59(1): 21–23.
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |