
![]()
A Man of Singular Vision
aka Ophthalmology Befuddler 026
A 52 year-old man presents with sudden onset loss of vision in his right eye. He has no other symptoms. His past medical history is notable for hypertension, hyperlipidemia and angina. His medications include aspirin, atenolol, and atorvastatin. He can barely detect hand movements with his right eye and has a relative afferent pupillary defect.
Fundoscopy shows this appearance:

Questions
Q1. What is the likely diagnosis?
Answer and interpretation
Central retinal artery occlusion (CRAO)
The diagnosis must be suspected in any case of sudden painless loss of vision, and is clinched by the appearance of the retina (see Q2).
Q2. What features on history and examination should be looked for?
Answer and interpretation
History:
- sudden and painless loss of vision (seconds)
- Consider underlying causes: emboli, thrombosis, GCA, CTDs, hypercoagualtion, trauma, migraine, syphilis, sickle cell disease, Behcet
Examination:
- Visual acuity — markedly reduced e.g. <6/60
- Marcus-Gunn pupils (RAPD)
- Red reflex — abnormal and asymmetrical
- Fundoscopy — a pale retina with areas of cilioretinal sparing and a classic ‘cherry red spot’ in the macula (may be subtle). Arteriolar and venular narrowing and box-car appearance
Q3. What is the investigation and management?
Answer and interpretation
CRAO, like chemical injuries to the eyes, is a true ophthalmological emergency.
Urgent ophthalmology referral, and a physician to work up underlying causes:
- Urgent ESR and CRP to exclude GCA.
- TIA and vasculitis work up as per amaurosis fugax
Treatment is unproven but includes:
- immediate ocular massage
- anterior chamber paracentesis
- IOP reduction with acetazolamide (e.g. 500mg IV) or timolol (0.5% topical drops bd)
- Breathe into a paper bag (respiratory acidosis induces retinal vasodilation)
Q4. How does an ophthalmic artery occlusion differ from this condition?
Answer and interpretation
There is no cherry red spot and vision is reduced to light perception. The entire retina is whitened. The treatment is the same.
Now, consider an alternative scenario in which the patient only had partial visual field loss and you saw this on funduscopy:
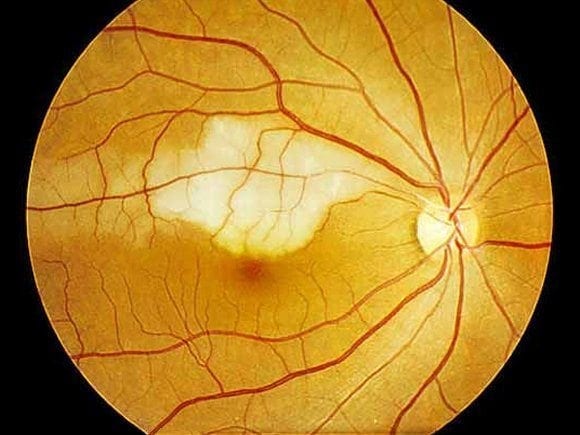
Q5. What is the diagnosis in this case, and how does it differ from the first?
Answer and interpretation
Branch retinal artery occlusion (BRAO)
There is no cherry red spot and there is only partial visual field loss. A segment of retina is whitened along the distribution of a branch retinal artery. The treatment is the same.
References
- Ehlers JP, Shah CP, Fenton GL, Hoskins EN. The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease Lippincott Williams & Wilkins
- NSW Statewide Opthalmology Service. Eye Emergency Manual — An illustrated Guide. [Free PDF]

OPHTHALMOLOGY BEFUDDLER
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC