
![]()
Activate or Wait – 001
46-year-old male with one hour of central crushing chest pain. Background of hypertension, morbidly obese and a heavy smoker.
We are four minutes from your tertiary centre.
Would you activate your cath lab/STEMI protocol?
0
ECG Interpretation
What is your interpretation?
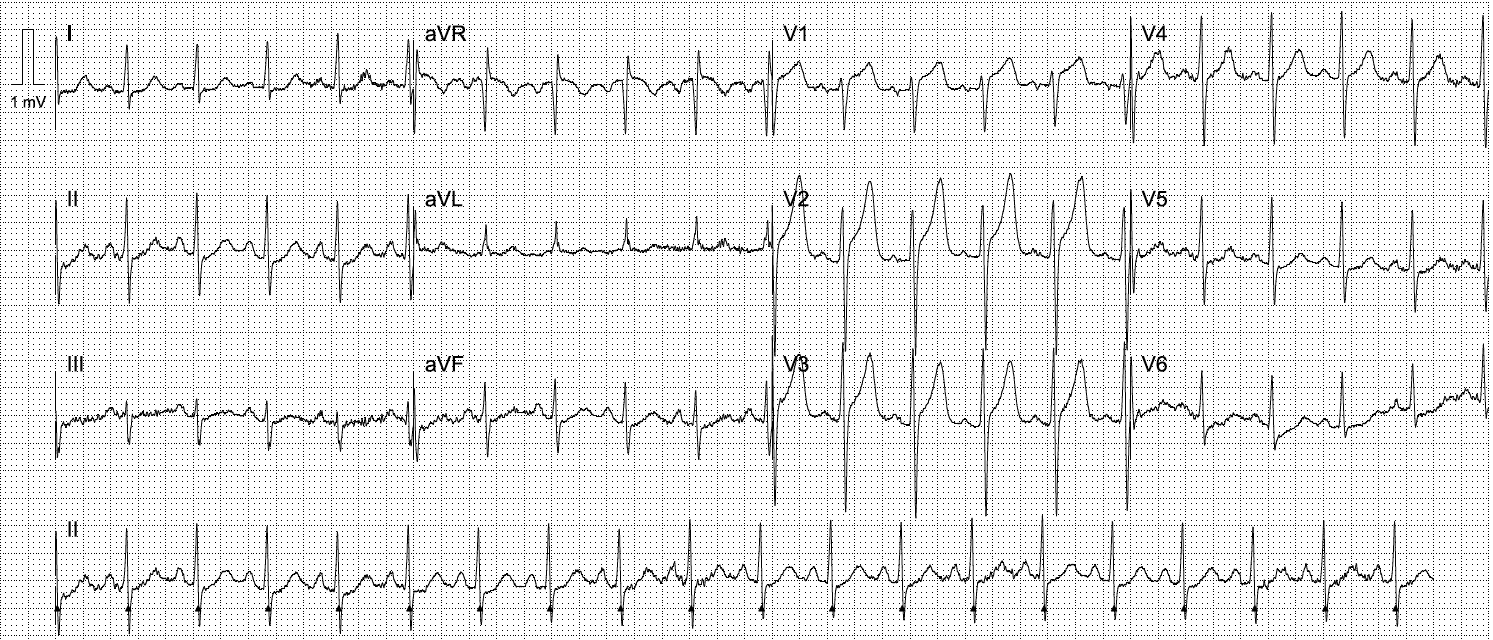
Anteroseptal STEMI
- Previously seen ST elevation in leads V1-3 is now significantly more pronounced, meeting traditional “STEMI” criteria
- Inferolateral ST depression is more prominent
ST elevation in aVR adds little diagnostic value here. It is most likely a reflection of diffuse subendocardial ischaemia, due to a combination of evolving infarction, tachycardia +/- hypotension (we are not given a blood pressure). Although infarction of the basal septum can cause ST elevation in aVR, we already suspect the above changes are secondary to left anterior descending artery (LAD) occlusion.
Take a deep dive into the misnomer of ST elevation in aVR.
ECG interpretation
Evolving anteroseptal occlusion myocardial infarction (OMI)
- Prominent ST elevation in leads V1-3
- Reciprocal inferolateral ST depression in leads II, aVF, V5-6
- Asymmetric, peaked anterior T waves in V2-3 are quite atypical for occlusion and resemble a benign early repolarisation pattern. However, we should never diagnose early repolarisation when ST depression is present in any lead other than aVR
- Sinus tachycardia is likely secondary to pain and ischaemia
This ECG appearance has been recently termed precordial swirl, and is highly specific for
LAD occlusion (see clinical pearls below). The degree of ST elevation often fails to meet
traditional STEMI criteria.
Given proximity to arrival, no activation call was made. The cardiology team met the patient on arrival and a second ECG was performed:

AI interpretation by PMcardio
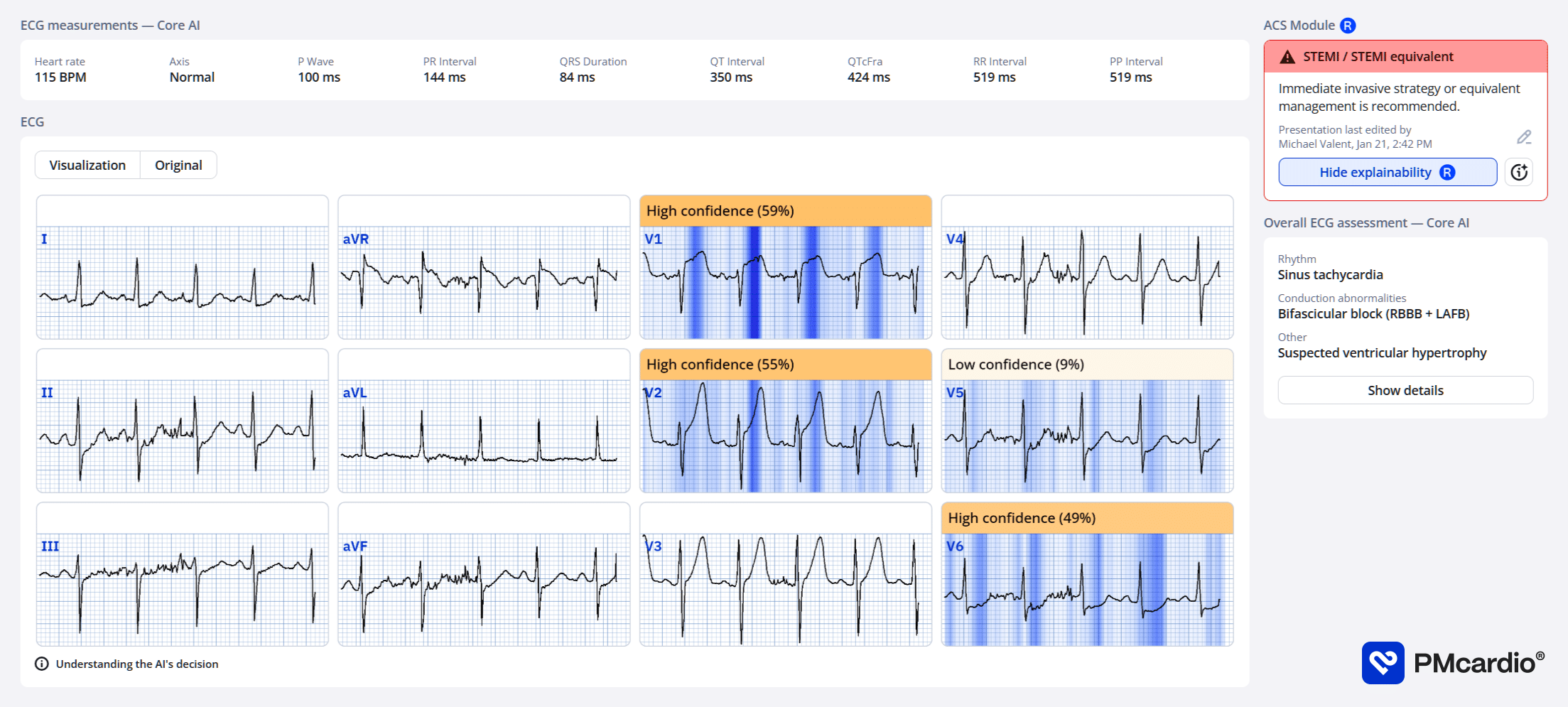
PMcardio’s AI ECG model identified a STEMI/STEMI equivalent.
The explainability feature offers insights into problematic patterns in the respective leads, providing a clear rationale for the diagnosis.
Further reading
Outcome
This patient was taken for emergent angiography.
Key Finding:
Occluded proximal LAD
Findings:
- Left Main Coronary Artery – Normal
- Left Anterior Descending Coronary Artery – Occluded proximally. Type III vessel.
- Left circumflex coronary artery – Large calibre vessel. Co-dominant. Mild irregularities.
- Right coronary artery- Small calibre vessel. Co-dominant. Mild diffuse disease.
Conclusion:
- Single vessel coronary artery disease. Occluded LAD.
- Proceeded to percutaneous coronary intervention to LAD.
Recommendation:
Admit CCU
Dual antiplatelet therapy – aspirin 100mg + ticagrelor 90mg BD for 12 months. Aspirin 100mg daily for life
Ongoing aggressive cardiovascular risk factor management
Smoking cessation
Clinical Pearls
- ST elevation can be subtle in the early stages of occlusion myocardial infarction. Always examine closely for ST depression and wide, bulky T waves. Remember, area under the curve is more important than overall height in hyperacute T waves
- ST elevation in aVR is simply a reciprocal change to widespread ST depression resulting from subendocardial ischaemia. Always consider non-cardiac causes (hypotension, hypoxia)
References
Further reading
- Smith SW. Precordial Swirl – 20 cases of Swirl or Look-Alikes. Dr Smith’s ECG blog
- Buttner R, Burns E. Anterior Myocardial Infarction. LITFL
- Nickson C. STEMI Management. LITFL
- Burns E, Buttner R. T wave. LITFL
Online resources
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
ACTIVATE or WAIT
EKG Interpretation

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Dr. Stephen W. Smith is a faculty physician in the Emergency Medicine Residency at Hennepin County Medical Center (HCMC) in Minneapolis, MN, and Professor of Emergency Medicine at the University of Minnesota. Author of Dr Smith's ECG Blog | Bibliography | X |

Dr. Robert Herman is the Co-founder and Chief Medical Officer of PMcardio by Powerful Medical. He is a cardiovascular researcher at the Cardiovascular Center Aalst in Belgium, specializing in applying AI to enhance the detection and referral of cardiovascular patients. LinkedIn | X (formerly Twitter) | Get in Touch

Great addition team! I hope 100 cases is the goal!