
![]()
Activate or Wait – 008
52-year-old male, previously well, one hour of central chest pain radiating to the back. BP 80/45.
We are 10 minutes from your tertiary centre.

Would you activate your cath lab/STEMI protocol?
0
ECG interpretation
Diffuse subendocardial ischaemia due to oxygen supply-demand mismatch. This ECG pattern is rarely caused by acute coronary occlusion
- Widespread ST depression in leads V2-6, I, II, III, aVF
- Reciprocal ST elevation in aVR
- No Q waves
- No ST elevation in V1-2 that would suggest septal infarction
ST elevation in aVR is a reciprocal change to the widespread ST depression of subendocardial ischaemia, usually most prominent in I, II and V4-6. This is the same ECG pattern seen in patients with a positive stress test.
Oxygen supply-demand mismatch causing subendocardial ischaemia can be due to both cardiac and/or non-cardiac causes:
- Severe triple vessel disease
- LMCA or LAD insufficiency
- Hypotension
- Hypoxia
- ROSC post cardiac arrest
Patients will often have a combination of the above – shock due to sepsis or hypovolaemia may unmask underlying coronary artery insufficiency. Examine other leads closely for changes suggestive of concurrent occlusion myocardial infarction (OMI):
- ST elevation in V2-4 suggestive of anterior OMI
- Isolated ST elevation in lead III suggestive of inferior OMI (Aslanger pattern)
- ST depression maximal in V1-3 that suggests posterior OMI
In the absence of these above changes, acute coronary occlusion is rarely the cause of this ECG pattern. These authors would suggest cardiology review on arrival and strong consideration of non-occlusive causes of ST elevation in aVR. Accredited bedside echo may be useful in guiding initial workup.
AI interpretation by PMcardio
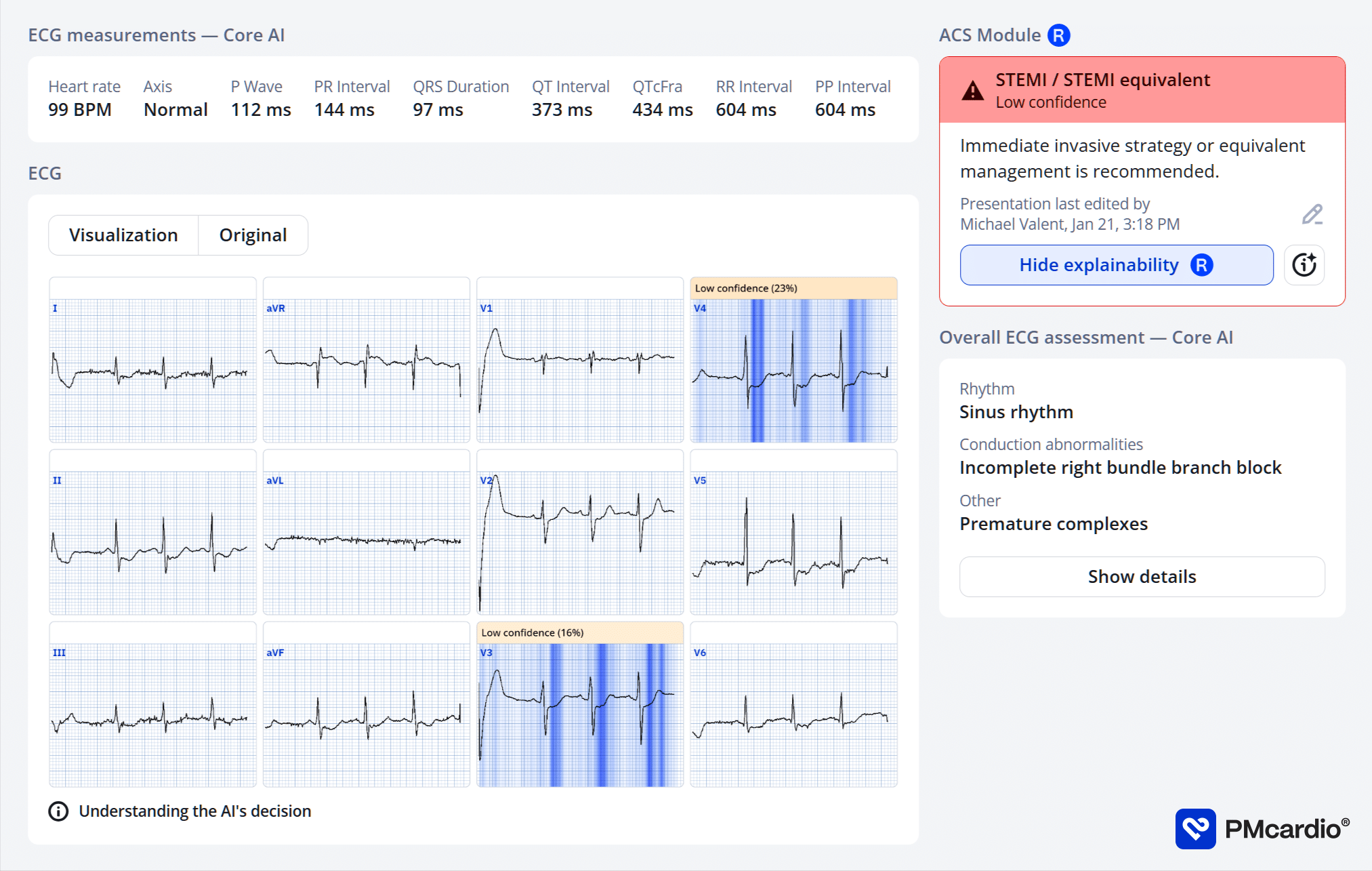
PMcardio’s AI ECG model identified a STEMI/STEMI equivalent.
The explainability feature offers insights into problematic patterns in the respective leads, providing a clear rationale for the diagnosis.
Further reading
Outcome
Key Finding:
Evidence of dissection flap and severe aortic regurgitation
Findings:
- Left Main Coronary Artery – Normal
- Left Anterior Descending Coronary Artery – Normal
- Left Circumflex Coronary Artery – Normal
- Right Coronary Artery – Normal
- Aortogram – Evidence of dissection flap and severe aortic regurgitation
Plan:
- CTS referral made urgently
- Patient transferred to CT then to OT
Clinical Pearls
In the absence of ST elevation elsewhere, ST elevation in aVR is usually NOT indicative of occlusion. The best way to differentiate between cardiac and non-cardiac etiologies is the clinical presentation – tachycardia, hypoxia, hypotension without severe LV dysfunction, or fever all point towards non-cardiac causes. Always consider and correct these causes.
In patients with suspected ACS, ST elevation in aVR and diffuse ST depression warrants early discussion with cardiology and prompt (within 24-48 hours) angiography.
References
Further reading
- Harhash AA, Huang JJ, Reddy S, Natarajan B, Balakrishnan M, Shetty R, Hutchinson MD, Kern KB. aVR ST Segment Elevation: Acute STEMI or Not? Incidence of an Acute Coronary Occlusion. Am J Med. 2019 May;132(5):622-630.
- Knotts RJ, Wilson JM, Kim E, Huang HD, Birnbaum Y. Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? J Electrocardiol. 2013 May-Jun;46(3):240-8.
- Burns E, Buttner R. ST Elevation in aVR. LITFL
Online resources
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Smith SW. Dr Smith’s ECG blog.
- Rawshani A. Clinical ECG Interpretation ECG Waves
ACTIVATE or WAIT
EKG Interpretation

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Dr. Stephen W. Smith is a faculty physician in the Emergency Medicine Residency at Hennepin County Medical Center (HCMC) in Minneapolis, MN, and Professor of Emergency Medicine at the University of Minnesota. Author of Dr Smith's ECG Blog | Bibliography | X |

Dr. Hana Hybasek Dzurikova, MRCVS, PGCert MEd is a medical educator driving innovation and change in health professions education through technology-enhanced learning.
