
![]()
Citalopram overdose
aka Toxicology Conundrum 017
Your next patient is a 26 year-old female who claims to have ingested 40 x citalopram hydrobromide tablets (40mg each) about 3 hours ago. She appears anxious with a heart rate of 95/min. She is alert, orientated and has bilaterally equal 4mm pupils. Further examination is unremarkable.
Questions
Q1. Describe the toxicodynamics and toxicokinetics of citalopram.
Answer and interpretation
Toxicodynamics:
- Citalopram is a selective serotonin re-uptake inhibitor (SSRI). SSRIs are thought to primarily mediate their therapeutic and toxic effects by inhibiting serotonin re-uptake, which leads to increased central serotonergic neurotransmission.
- Citalopram is considered one of the most potent of the SSRIs, and its metabolites may cause QT prolongation.
- SSRIs bind other receptors only with low affinity (such as adrenergic, dopaminergic, cholinergic, serotonergic and histamine receptors).
Toxicokinetics:
- Absorption: Citalopram, like most SSRIs, is well absorbed following oral administration. Peak serum levels are reached at about 4 hours.
- Distribution: 80% protein bound (including metabolites) with a large volume of distribution (~12 L/kg).
- Metabolism: hepatic metabolism (CYP3A4 and CYP2C19 N-demethylation) produces metabolites with lower activity and higher water solubility. Citalopram has a metabolite called didesmethylcitalopram (DDCT) that causes QT prolongation. Other metabolites include demethylcitalopram (DCT), citalopram-N-oxide, and a deaminated propionic acid derivative.
- Elimination: elimination half-life is about 35 hours. 10% is renally excreted unchanged.
Descriptions of the toxicodynamics and toxicodynamics of drugs should be taken with a grain salt – in large overdoses, drugs often don’t do things by the book…
Q2. What is the risk assessment for this patient?
Answer and interpretation
This patient has ingested a large amount (1600 mg) of citalopram. The risk assessment is:
Severity of serotonin toxicity can be variable.
- Higher severity is expected if the patient has coingested other serotonergic drugs and in very large overdoses.
- Mild symptoms usually begin within 4 hours. They typically consist of nausea, anxiety, tachycardia or bradycardia, sweating, and mydriasis.
- Serotonin toxicity classically has a time course of about 12 hours (<24 hours). However, in large ingestions – particularly if there are serotonergic coingestants, delayed gastric absorption (e.g. pharmacobezoar formation or ileus due to anticholinergic coingestants), or other concomitant illness (e.g. sepsis) the syndrome may be prolonged.
- Seizures are uncommon (2-4%). They are usually brief and responsive to benzodiazepines. Warning signs of an imminent seizure include increased anxiety, sweating, tremor, tachycardia and mydriasis.
- Coma is not a sign of serotonin toxicity – consider the possibility of an alternative diagnosis, the presence of complications (e.g. hypoxic or hyperthermic encephalopathy) or coingestion of other drugs.
Risk of QT prolongation is dose-dependent in citalopram overdose.
- may be delayed as it is primarily caused by the DDCT metabolite.
- overall about 2/3 cases of citalopram overdose have a QTc >440 ms and about 1/8 cases have QTc >500 ms.
- Risk of significant QT prolongation occurs with overdoses of 600mg or higher.
- Cardiac dysrhythmias (such as torsades de pointes (TdP)) are rarely reported.
Q3. Describe measurement of the QT interval and calculation of the rate-corrected QT (QTc) interval.
Answer and interpretation
The QT interval is the ECG manifestation of ventricular depolarization and repolarization. It is measured from QRS complex onset to T wave termination. Because QT intervals normally shorten with tachycardia and lengthen with bradycardia, is common practice to calculate a rate-corrected QT (QTc) interval.
The Bazett formula is widely used for this purpose:
- Bazett Correction: QTc = QT / (RR)1/2
A problem with Bazett’s correction is that it tends to over-correct QT at fast heart rates (>70 bpm) and under-correct QT interval at slow heart rates (<50 bpm). Thus overdoses associated with drugs such as quetiapine, that are associated with tachycardia, tend to result in long QTc’s, and the risk of true cardiotoxicity is probably over-estimated.
Alternative corrections that have been proposed are:
- Fridericia Correction: QTc = QT / (RR)1/3
- Framingham Correction: QTc = QT + 0.156 x (1-RR)
Charbit B et al in a study of 108 patients found that automatic QT correction using Bazett formula had a sensitivity for detection of QT prolongation of 54% while automatic QT correction using Fridericia formula had 100% sensitivity
Q4. What degree of QT prolongation is of concern?
Answer and interpretation
This is highly controversial and remains poorly defined. As a fairly arbitrary rule of thumb, we consider a QTc >450 ms as mandating continuous cardiac monitoring due to the risk of TdP.
However, TdP is less likely if the patient is relatively tachycardic, with most drug-induced cases occurring at relatively slow heart rates. There is also considerable inter-individual variation – in that the risk of life-threatening dysrhythmia varies between different people with the same degree of QT prolongation.
Q5. What is the best method of assessing QT prolongation in a toxicological setting?
Answer and interpretation
The widely used Bazett’s correction is the “gold standard”. Yet, although QT prolongation is clearly associated with an increased risk of TdP, there is no reliable criterion to identify the length of QT prolongation that is associated with a clinically significant increased risk of TdP. Because of significant inter-individual variation in the risk of life-threatening dysrhythmia for a given QT interval, an individually based assessment of risk may be most accurate. However, this is generally not feasible in clinical settings.
Chan et al (2007) have evaluated an approach to the assessment of pro-arrhythmic risk in QT prolongation using a nomogram, which does not require the use of correction formulas or numerous previous ECGs required for individual HR correction. This nomogram is based on a ‘QT–RR cloud diagram’ developed from human preclinical studies. Chan et al’s analysis suggests that their nomogram outperforms Bazett’s correction for predicting pro-arrhythmic risk, with sensitivities and specificities >96.9%.
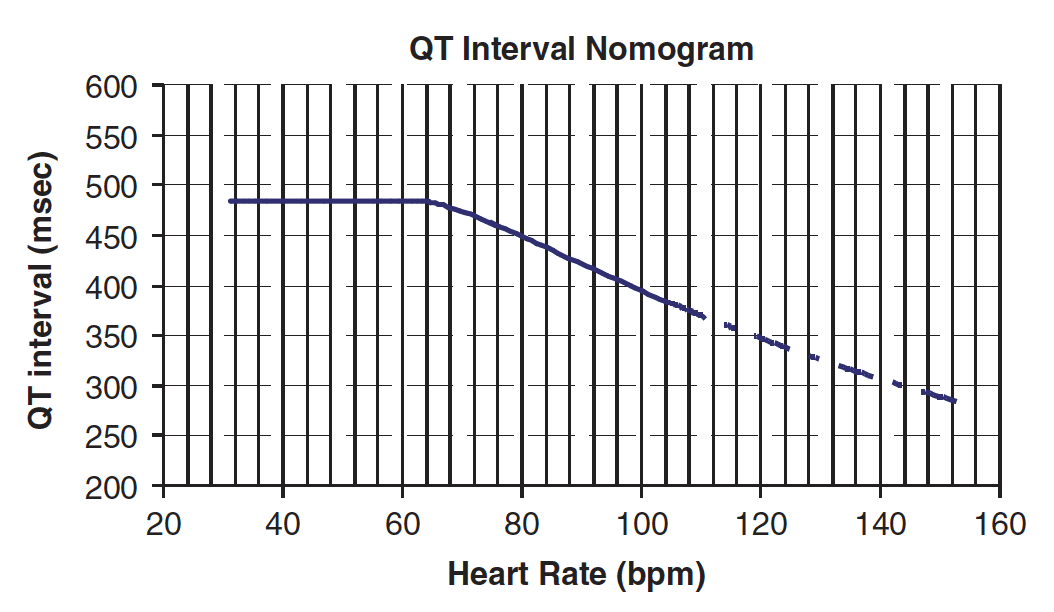
The nomogram is used as follows:
“The QT interval should be measured manually on a 12-lead ECG from the beginning of the Q wave until to the end of the T wave in multiple leads (i.e. six leads including limb and chest leads and median QT calculated). The QT interval is plotted on the nomogram against the heart rate recorded on the ECG. If the point is above the line then the QT–HR is regarded ‘at risk’.” – Chan et al, 2007.
Q6. Describe the management of this patient with a citalopram overdose.
Answer and interpretation
Using the “Resus-RSI-DEAD” approach:
- Resuscitation, supportive care and monitoring –
Assess and support ABC’s.
Seizures and agitation – treat with titrated benzodiazepines. If increasing anxiety, sweating, tremor, tachycardia and mydriasis occurs pre-emptively treat with IV diazepam 5mg every 2-5 minutes until gentle sedation is achieved, as these features may herald the onset of seizures.
Serotonin syndrome – features of serotonin toxicity respond well to titrated benzodiazepines. Other pharmacologic treatment options include cyproheptadine, chlorpromazine and olanzepine. Consider intubation and neuromuscular paralysis if marked rigidity, PaCO2 is rising, CK is rising or hyperthermia (T>39.5 C) is present.
Torsades de pointes (TdP) – treat with oxygen, magnesium chloride 10 mmol IV, correct hypokalemia, and consider overdrive transcutaneous pacing (HR 120/min) or treatment with either isoprenaline, adrenaline or dopamine. If the patient is pulseless then DC cardioversion (~200J biphasic) and CPR is indicated. - Risk assessment – See Q2.
- Investigations –
Screening tests – ECG at presentation, glucose, paracetamol level.
Serial 12-lead ECGs – continuous ECG monitoring is performed for at least 13 hours if >1000 mg citalopram is ingested (8 hours if between 600mg and 1000mg is ingested). If QTc is <450ms on a 12-lead ECG at the end of this period ECG monitoring may be ceased. - Decontamination –
50g activated charcoal can be administered to alert and cooperative patients who have ingested >600mg of citalopram.
NB. Activated charcoal is not indicated for other SSRIs that do not cause QT prolongation – as outcomes are good with supportive care only). - Enhanced elimination and antidotes – Nil.
- Disposition –
The patient requires cardiac monitoring for a minimum of 13 hours (as the ingested dose is >1000mg, if 600-100mg then 8 hours is sufficient), and may be discharged at this time (following psychiatric clearance) if she is asymptomatic with a QTc <450 ms.
If features of serotonin toxicity are present supportive care in a ward environment for 12 to 24 hours is typically required until they resolve.
Severe serotonin toxicity and dysrhythmias require ICU level care.
Q7. Would the risk assessment and management plan change if the patient ingested escitalopram instead of citalopram?
Answer and interpretation
Escitalopram is the S-enantiomer of citalopram. It is a more potent inhibitor of the serotonin transporter and is probably responsible for most of the SSRI effect in racemic citalopram. Clinical experience in escitalopram overdose has been relatively limited, although a series of 79 cases was recently published (van Gorp et al, 2009) .
Overall, it appears reasonable to manage escitalopram overdose in a similar way to citalopram. The major manifestations of escitalopram overdose are serotonin toxicity, QT prolongation, and bradycardia. The risk of cardiac arrhythmias according to QT intervals appear similar to that with citalopram. Of note, no cases of seizures or life-threatening dysrhythmias were reported in van Gorp et al’s case series of escitalopram overdose (note that the maximum dose ingested was only 560 mg).
References
- Chan A, Isbister GK, Kirkpatrick CMJ, Duffu SB. Drug-induced QT prolongation and torsades de pointes: evaluation of a QT nomogram. QJM 2007 100(10):609-615 [fulltext]
- Friberg LE, Isbister GK, Duffull SB. Pharmacokinetic-pharmacodynamic modelling of QT interval prolongation following citalopram overdoses. Br J Clin Pharmacol. 2006 Feb;61(2):177-90. PMID: 16433872
- Friberg LE, Isbister GK, Hackett LP, Duffull SB. The population pharmacokinetics of citalopram after deliberate self-poisoning: a Bayesian approach. J Pharmacokinet Pharmacodyn. 2005 Aug;32(3-4):571-605. PMID: 16307209
- Isbister GK, Friberg LE, Stokes B, Buckley NA, Lee C, Gunja N, Brown SG, MacDonald E, Graudins A, Holdgate A, Duffull SB. Activated charcoal decreases the risk of QT prolongation after citalopram overdose. Ann Emerg Med. 2007 Nov;50(5):593-600, 600.e1-46. Epub 2007 Aug 23. PMID: 17719135
- Isbister GK, Friberg LE, Duffull SB. Application of pharmacokinetic-pharmacodynamic modelling in management of QT abnormalities after citalopram overdose. Intensive Care Med. 2006 Jul;32(7):1060-5. PMID: 16791669
- Isbister GK, Bowe SJ, Dawson A, Whyte IM. Relative toxicity of selective serotonin reuptake inhibitors (SSRIs) in overdose. J Toxicol Clin Toxicol. 2004;42(3):277-85. PMID: 15362595
- van Gorp F, Whyte IM, Isbister GK. Clinical and ECG effects of escitalopram overdose. Ann Emerg Med. 2009 Sep;54(3):404-8. Epub 2009 Jun 25. PMID: 19556032
- Bazett formula for QT correction [Henry Cuthbert Bazett (1885 – 1950)]
- Fridericia Formula for QT correction [Louis Sigurd Fridericia (1881-1947)]

CLINICAL CASES
Toxicology Conundrum
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC