
![]()
Clozapine toxicity
Clozapine is an atypical antipsychotic, due to its restricted use an acute overdose is a rare event but clinicians should be aware that coma can occur and management is with supportive care. In chronic toxicity agranulocytosis and myocarditis can occur, these are not features of an acute poisoning but monitored in patients with long term therapeutic use.
Toxic Mechanism:
Clozapine is an antagonist to dopamine (D1 and D2 in the mesolimbic system), serotonin, peripheral alpha receptors, muscarinic, histamine and GABA receptors. This combination of antagonism results in CNS depression, tachycardia, orthostatic hypotension and anticholinergic toxidrome.
Toxicokinetics:
- Rapidly absorbed
- Highly protein bound with a moderate volume of distribution 0.5 – 3 L/Kg.
- Metabolised in the liver and excreted in the urine
- Significant first-pass effect
Resuscitation:
- Reduced GCS: Prompt intubation and ventilation
- Hypotension: Give 10 – 20 ml/kg of IV crystalloid, patients usually respond to this.
- Seizures: IV benzodiazepines incrementally dosed every 5 minutes to effect.
- Can be managed with benzodiazepines (varying doses in the textbooks, easy method is 0.1mg/kg IV for lorazepam (max 4mg) / midazolam (max 10mg) / diazepam (max 10mg). Or…
- Lorazepam 0.1mg/kg max 4mg
- Diazepam 0.15mg/kg max 10mg
- Midazolam 0.2mg/kg max 10mg
Risk Assessment
- Severe poisoning including coma can occur with 100 mg in adults
- Toxicity is more likely to occur in those naive to the drug.
- Children: >2.5 mg/kg is associated with sedation and need hospital assessment (as little as one tablet). Extrapyramidal effects can occur in the days following.
- Clinical features normally manifest within 4 hours and toxicity is expected to resolve within 24 hours:
- Sedation, CNS depression leading to coma
- Tachycardia, common to be able 120 bpm
- Orthostatic hypotension
- Mild to moderate anticholinergic toxidrome (agitation, ileus, urinary retention)
- Mydriasis and miosis are both seen
- Hyper salivation is considered pathognomonic
- Seizures in 5 – 10% of patients
- QT prolongation is rare
Supportive Care
- Controlling the delirium can be difficult, things to consider include
- Titrated doses of benzodiazepines e.g. diazepam 2.5 – 5 mg every 5 minutes IV until gentle sedation is achieved
- Physical restraint
- Bladder scan and a catheter for urinary retention (no amount of benzodiazepines will fix this agitation)
Investigations
- Screening: 12 lead ECG, BSL, Paracetamol level
- Specific:
- ECG monitoring, do an ECG at presentation and 6 hours, if this is normal then cardiac monitoring may stop. If the QT >450 ms, monitoring should continue until the patient is clinically well and the ECG changes have resolved. Reports of minor QT prolongation but no Torsades de pointes.
- Clozapine levels are available, not useful in guiding clinical management but can help confirm the diagnosis.
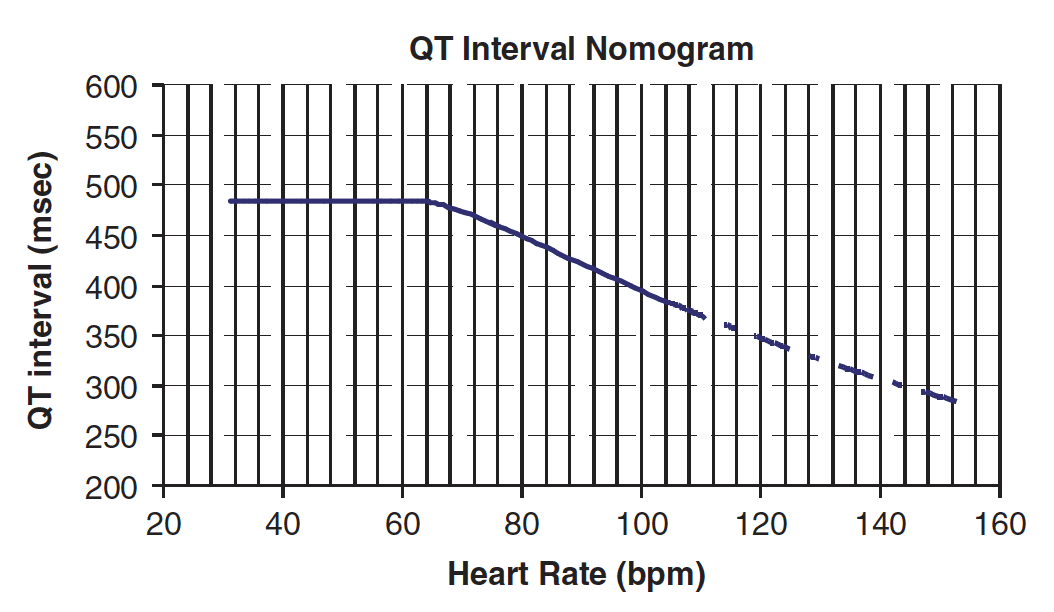
QT Nomogram
[/DDET]
Decontamination:
- 50g of activated charcoal is usually not indicated because of good supportive care. If the patient is intubated then charcoal can be given via a nasogastric tube.
Enhanced Elimination
- Not clinical useful
Antidote
- None available
Disposition
- Patients who are clinically well at 6 hours maybe medically cleared.
- Patients who develop symptoms need admission for appropriate supportive care.
- Parents need to be advised that their child may develop extrapyramidal movements up to seven days later.
References and Additional Resources
Additional Resources:
- Seizures, sedation and saliva – Joe Rotella’s clozapine OD case
- Tox conundrum: A fumbling, Mumbling Mess
- Coma and small pupils
- EMI 020 – Anticholinergic song
References:
- Burns MJ. The pharmacology and toxicology of atypical antipsychotic agents. Clinical Toxicology 2001: 39(1);1-14.
- Cobaugh DJ, Erdman AR, Booze LL et al. Atypical antipsychotic medication poisoning; an evidence based consensus guideline for out-of-hospital medication poisoning. Clinical Toxicology 2007; 45:918-942
- Isbister GK, Balit CR, Kilham HA. Antipsychotic poisoning in young children: A systematic review. Drug Safety 2005; 26(11):1029-1044.
- Reith D, Monteleone JP, Whyte IM et al. Features and toxicokinetics of clozapine in overdose. Therapeutic Drug Monitoring. 1998; 20(1):92-97.
- Trenton A, Currier G, Zwemer F. Fatalities associated with therapeutic use and overdose of atypical antipsychotics. CNS Drugs 2003; 17(5):307-324.
- Wong DC, Curtis LA. Are 1 or 2 dangerous? Clozapine and olanzapine exposure in toddlers. The Journal of Emergency Medicine 2004; 27:273-277

Toxicology Library
DRUGS and TOXICANTS
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.