
![]()
CT Case 017
An 80yo male is brought in by ambulance following an MVA where he rear-ended another vehicle while driving at 50km/hr.
He has midline cervical spine tenderness with a palpable step deformity. He has complete loss of motor function to his lower limbs and reduced strength to upper limbs.
His vital signs are HR 40, blood pressure 90/45, temperature 35°C.
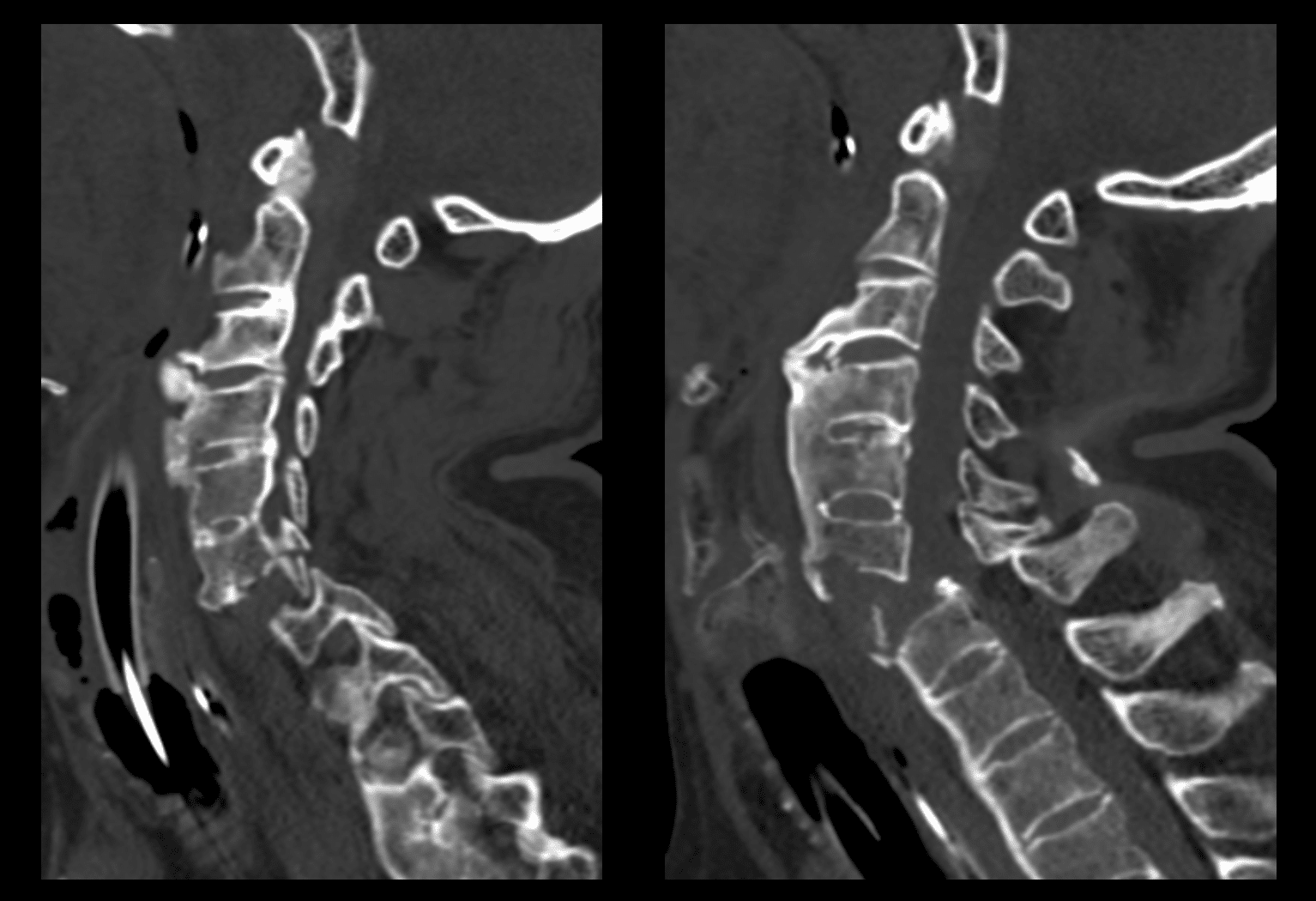
Describe and interpret the CT images
CT INTERPRETATION
There is a transverse fracture through the C6 vertebra.
There is 10mm of anterior displacement of C6 on C7 with associated bilateral C6/7 facet joint dislocation. This results in severe narrowing of the spinal canal.
There is also a comminuted fracture of the superior end-plate of C7.
There are prominent anterior bridging ossifications causing ankylosis of the cervical spine. The term ankylosis is used to describe abnormal immobility of a joint due to bony union. This same appearance was also seen on the lumbar and thoracic spine imaging for this patient.
This appearance is consistent with a pathological condition known as Forestier disease or DISH (Diffuse Idiopathic Skeletal Hyperostosis).

CLINICAL CORRELATION
This case demonstrates bilateral facet joint dislocation with associated fracture.
Bilateral facet joint dislocation is a highly unstable cervical spine injury resulting in narrowing of the spinal canal.
This patient has evidence of cord compression as a result of this injury.
This patient also has neurogenic shock. This is a loss of sympathetic tone sometimes seen in spinal cord injuries above the T6 level. Neurogenic shock causes vasodilation, bradycardia and poikilothermia (inability to maintain body temperature).
A diagnosis of neurogenic shock, is a diagnosis of exclusion, after eliminating other causes of hypotension in a trauma patient (ie, haemorrhage, tension pneumothorax and tamponade). Neurogenic shock is managed with judicious IV fluids and noradrenaline infusion.
DISH is a pathological process characterised by flowing calcification and ossification along the anterolateral aspect of at least four contiguous vertebral bodies. It results in fusion of vertebrae, and therefore causes reduced spinal column mobility. DISH typically occurs in the elderly, and has an association with diabetes and obesity.
A disease with a similar appearance is ankylosing spondylitis. However, it is actually an entirely different disease process. Ankylosing spondylitis is an inflammatory disorder, that typically develops in early adulthood. A key differentiator is the presence of sacroiliitis in ankylosing spondylitis, this is rarely seen in DISH.
The pathological changes that occur in both DISH with ankylosing spondylitis put patients at much higher risk of cervical spine fracture even with low energy trauma. As a result of the increased rigidity in DISH, the spine tends to fracture transversely involving multiple columns, leading to instability and not uncommonly translation. Important to note that these fractures can be subtle initially in some cases.
REFERENCES
- Cadogan M. Forestier disease. LITFL
[cite]
TOP 100 CT SERIES

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.