
![]()
Abdominal CT: intestinal ischaemia
Identifying intestinal ischaemia
Mesenteric ischaemia can be caused by any process that reduces intestinal blood flow and results in injury and inflammation to the bowel wall.
When it is due to vascular occlusion, mesenteric ischaemia typically presents with severe diffuse abdominal pain and and elevated lactate and white cell count.
There are a variety of imaging characteristics to be aware of based on where the blockage is and how quickly the patient undergoes imaging. In order to avoid missing this important diagnosis, you will need to carefully evaluate:
- Both the mesenteric arteries and veins for signs of clot formation or narrowing
- The bowel wall for thickness and enhancement
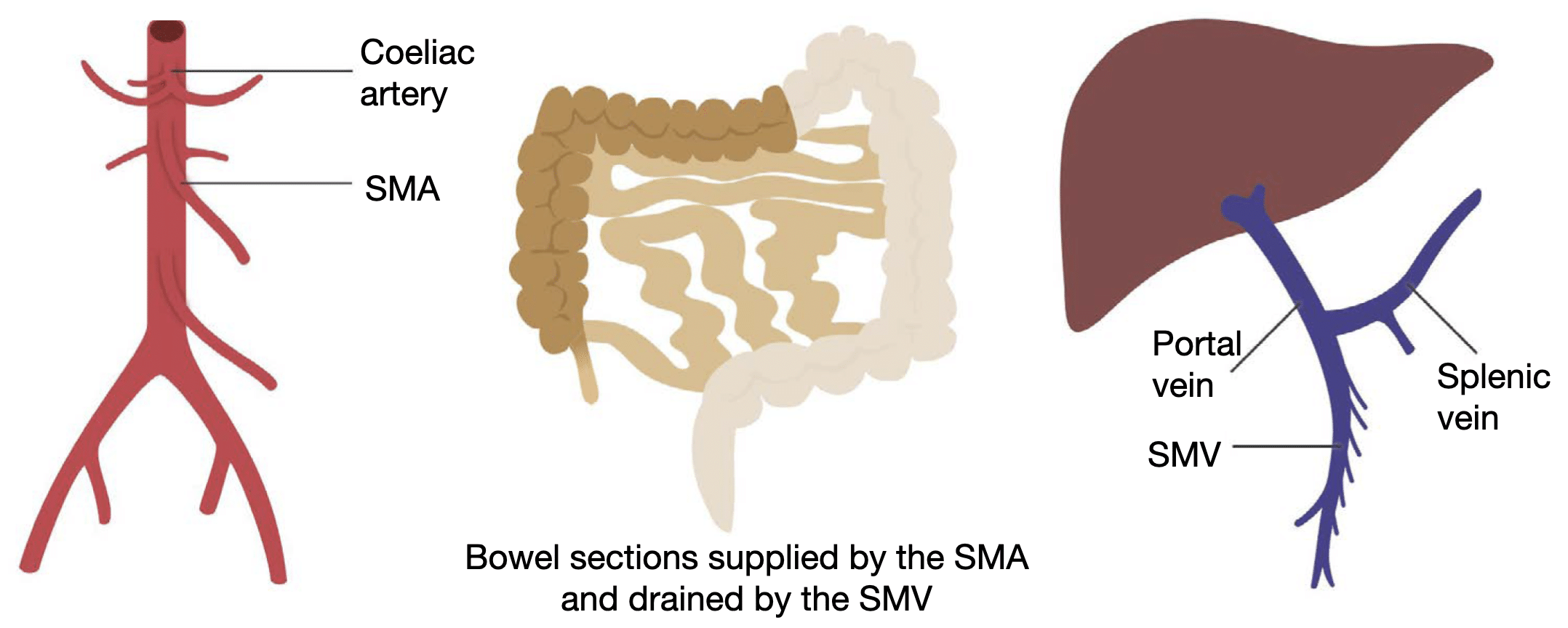
The Superior mesenteric artery (SMA) is the second major branch of the abdominal aorta after the coeliac artery. It supplies the small bowel and portions of the large bowel – specifically the cecum and ascending colon – through the ileocolic branches and part of the transverse colon through the middle colic branches.
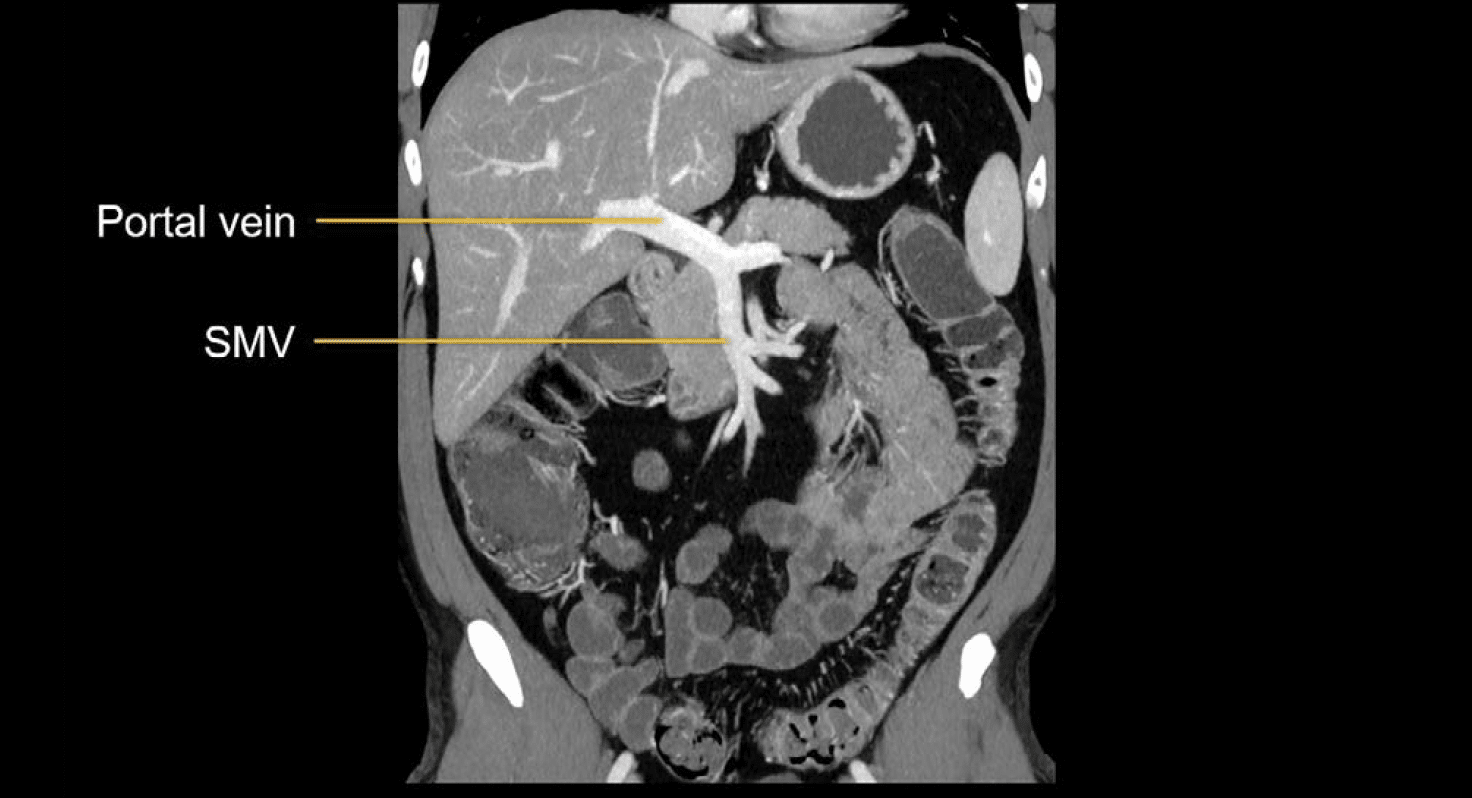
The superior mesenteric vein (SMV) drains the same bowel loops that are supplied by the superior mesenteric artery and, along with the splenic vein, forms the portal vein and drains into the liver.
Arterial ischaemia
Acute arterial occlusion is most commonly due to thromboembolic disease, which occurs when a clot becomes lodged in an artery and blocks the blood flow.
For mesenteric ischaemia, the most common site of blockage is the superior mesenteric artery. Such a blockage causes a rapid reduction in blood flow to the small bowel, resulting in tissue death. Surgical removal of the involved segment is often required.
Examining the arteries
If the occlusion is located near the start of the superior mesenteric artery, then a large portion of bowel will be involved, and you can often see the clot blocking the blood flow on the CT images.
Example 1
Sagittal image shows the relationship between the coeliac artery, superior mesenteric artery, and the abdominal aorta. The patient has bright calcified plaque throughout the aorta related to atherosclerosis. There is acute occlusion of the SMA proximally, and we can see an abrupt cutoff where the contrast in the vessel stops due to a clot.

In some cases, smaller clots will travel to distal branches and can be hard to see. In those settings, you would watch for abnormal enhancement of the bowel as the major sign of ischaemia
Examining the bowels
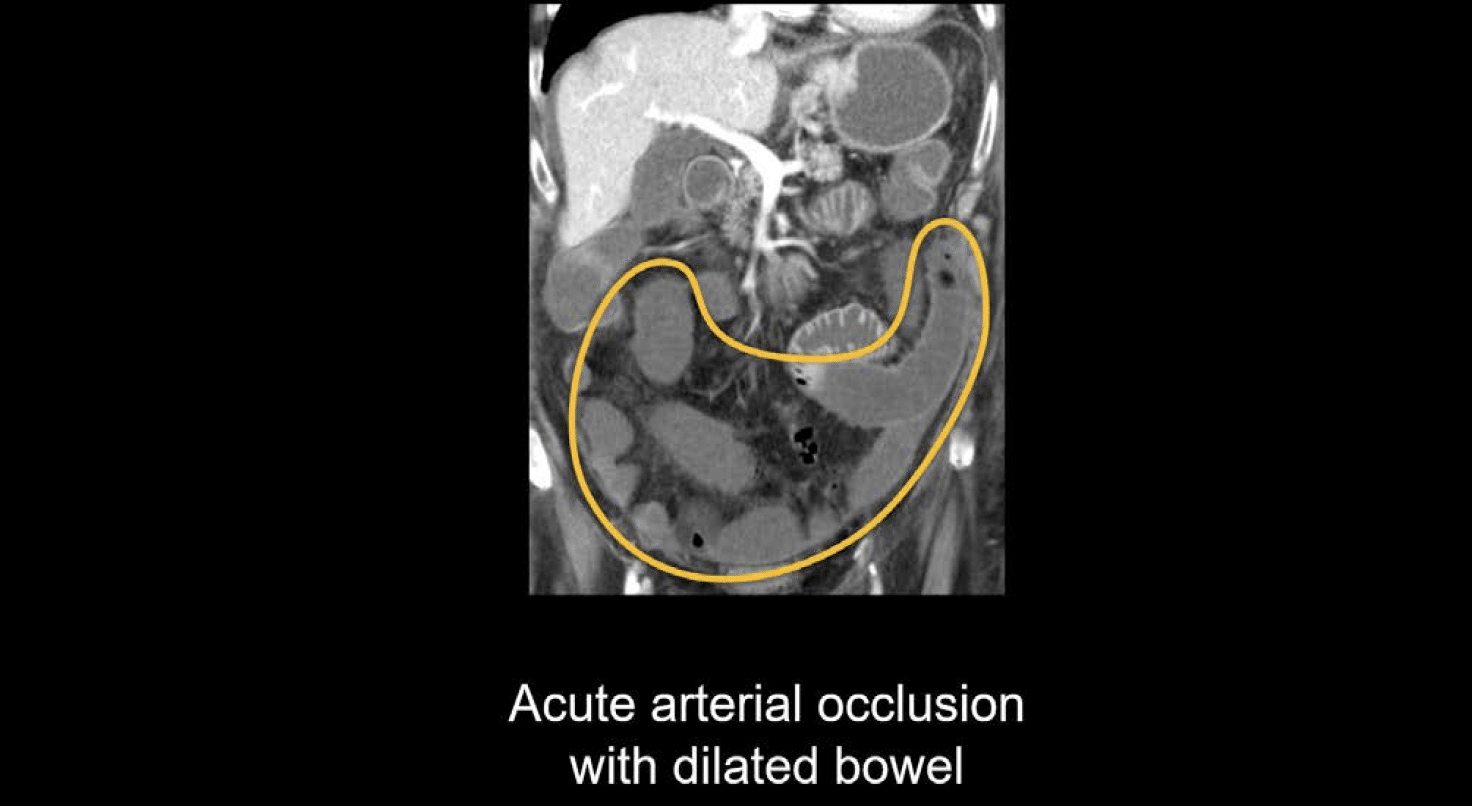
When there is an arterial occlusion, the bowel will look different depending on the severity and duration of the blockage. When blood flow is first blocked, you may notice that the bowel will first dilate; then the wall may become thin and enhance less; and there is usually little surrounding fluid.
There may be an abrupt cutoff of enhancement at watershed areas of vascular supply as in the example below where we can see a transition from enhancing to non-enhancing bowel.

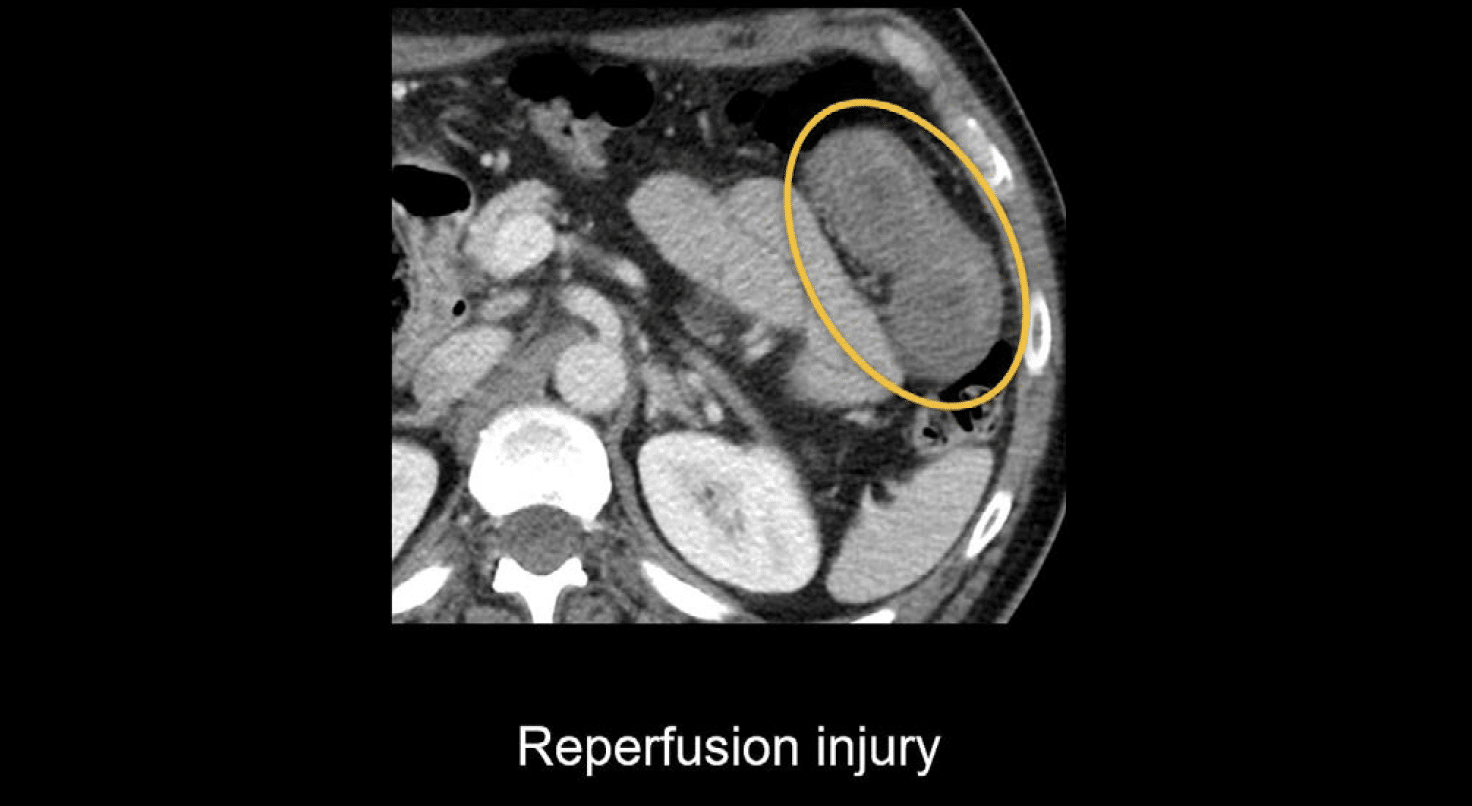
If blood flow is partially restored after ischaemia, you might see thickening of the wall. This is called a reperfusion injury, and it happens because the wall cannot handle the new blood flow after being ischaemic.
Another important sign of bowel iscahemia and wall damage is called pneumatosis, which occurs when gas forms in the bowel wall. The wall will typically be thickened and have lots of small black dots of air within it. This is even more apparent if we apply the lung window settings.

Knowledge iteration
Review a case of arterial ischaemia due to an acute occlusion of the superior mesenteric artery. This case was imaged with the mesenteric iscahemia protocol which includes both late arterial and portal venous phase imaging.
- Starting with the late arterial images, look at the abdominal aorta. You should notice quite a lot of atherosclerotic disease.
- The first branch is the celiac axis. The superior mesenteric artery is open proximally, but as you scroll distally, it stops enhancing because it is occluded.
- If you move on to the portal venous images, you’ll notice that much of the bowel is simply not enhancing. You can compare this to the duodenal sweep and proximal jejunal branches which are not occluded and have increased enhancement.
- When such a large amount of bowel is ischaemic, it can be difficult to notice what is enhancing and what is not! However, coronal images can help to highlight the enhancing versus ischaemic segments.
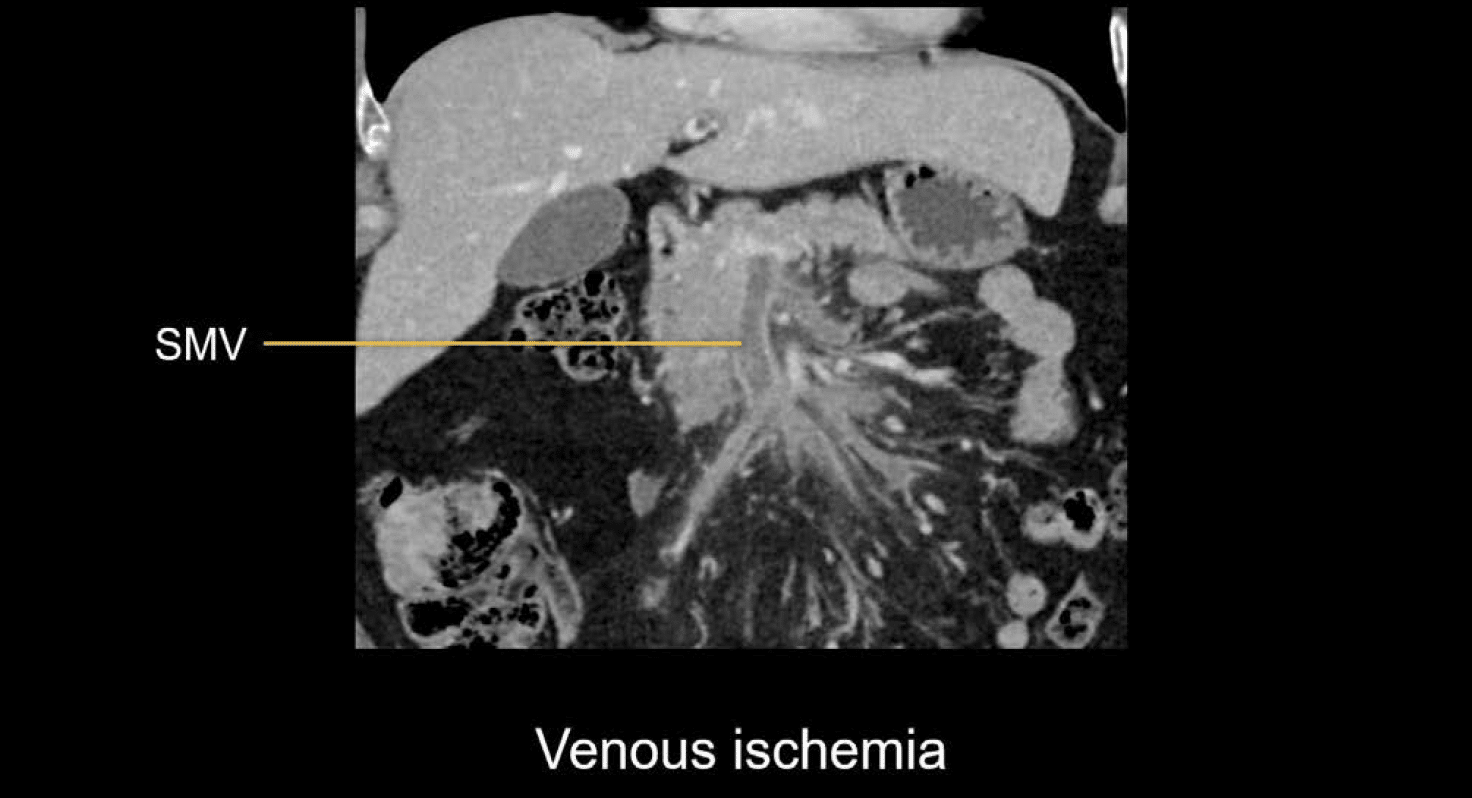
Venous ischaemia
Examining the veins
Venous ischaemia is due to thrombosis of the superior mesenteric and portal veins.
In contrast to arterial ischaemia, venous ischaemia does not often cause a quick death of the bowel tissue. Instead, venous ischaemia causes usually causes elevated venous pressures; bowel wall thickening; abnormal enhancement and fluid accumulation (resulting in a hazy, congested-looking mesentery)
The abnormal enhancement and fluid accumulation occur due to lymphatic congestion (which is caused by blockage of the venous outflow). As the artery keeps pumping blood, venous pressures increase, and this causes fluid to accumulate.
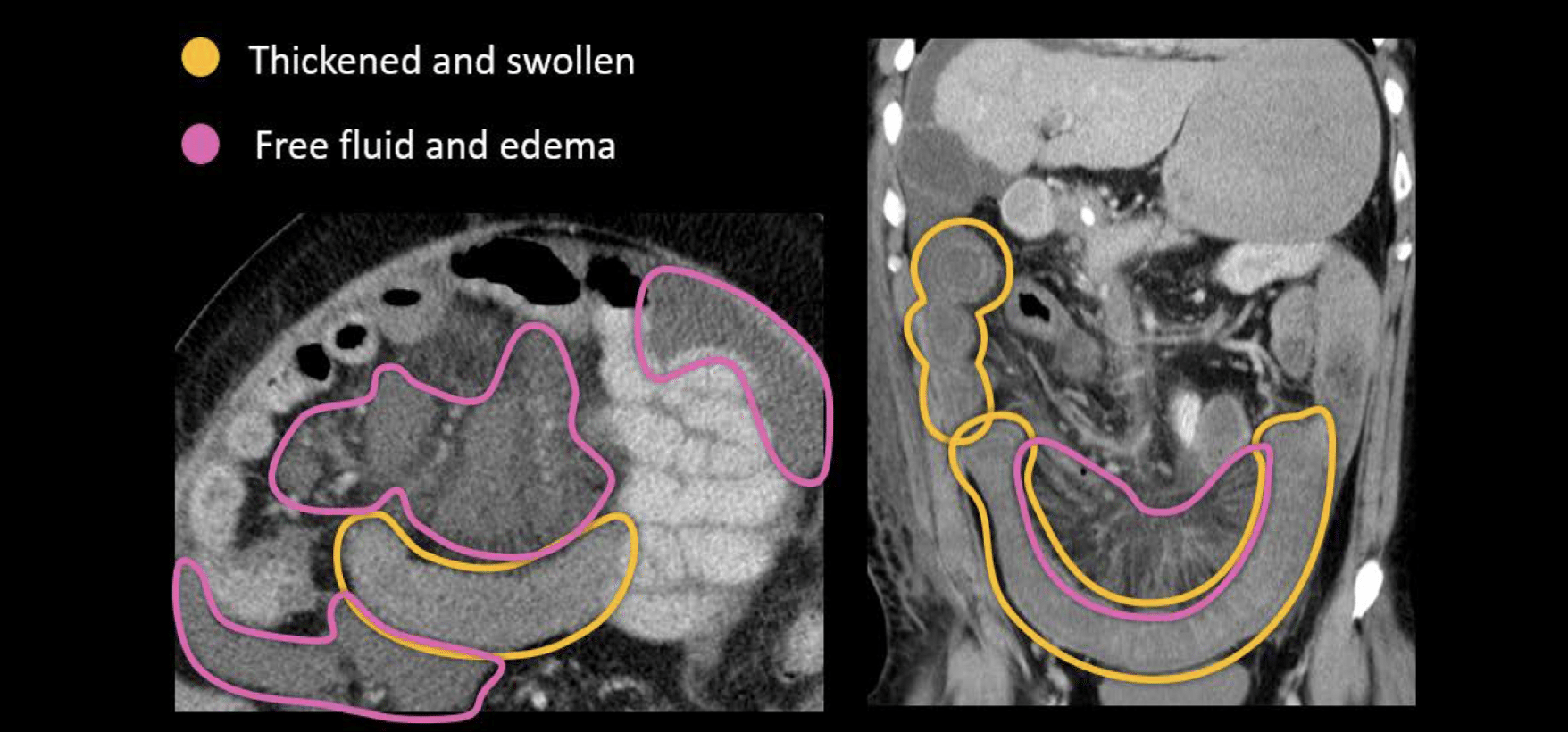
Examining the bowels
With venous ischaemia, we typically see:
- Thickened and swollen small bowel loops with relatively decreased enhancement
- Free fluid and oedema in the mesentery (due to increased venous pressures)
Knowledge iteration
Review the online PACS images from a patient who developed postoperative abdominal pain after having a portion of colon removed due to ulcerative colitis.
- As you scroll throughout the abdomen, notice that much of the small bowel is abnormally thickened.
- You can see the three layers of mucosal enhancement, submucosal oedema, and serosal enhancement, but they look a little decreased overall.
- There is ascites and congestion throughout the mesentery.
- You might think that this could be due to infection or peritonitis from the patient’s recent surgery, but there are no abscesses, and the peritoneal lining is not particularly thickened.
- By following the superior mesenteric vein, you will find that the entire course of the vein (including the portal and splenic veins) is filled with clotting, which confirms that venous ischaemia is the cause for this abnormally small bowel.
This is an edited excerpt from the Medmastery course Abdominal CT Pathologies by Michael P. Hartung, MD. Acknowledgement and attribution to Medmastery for providing course transcripts
- Hartung MP. Abdominal CT: Common Pathologies. Medmastery
- Hartung MP. Abdominal CT: Essentials. Medmastery
- Hartung MP. Abdomen CT: Trauma. Medmastery
References
- Top 100 CT scan quiz. LITFL
- Rippey J. Ultrasound Case 049. LITFL
Radiology Library: Acute abdomen. Solid organ and Vascular pathology
- Hartung MP. Abdominal CT: acute interstitial pancreatitis
- Hartung MP. Abdominal CT: acute necrotizing pancreatitis
- Hartung MP. Abdominal CT: renal stones and the flank pain CT
- Hartung MP. Abdominal CT: renal infections
- Hartung MP. Abdominal CT: cholecystitis
- Hartung MP. Abdominal CT: intestinal ischaemia
- Hartung MP. Abdominal CT: rupturing abdominal aortic aneurysm
Abdominal CT interpretation

Assistant Professor of Abdominal Imaging and Intervention at the University of Wisconsin Madison School of Medicine and Public Health. Interests include resident and medical student education, incorporating the latest technology for teaching radiology. I am also active as a volunteer teleradiologist for hospitals in Peru and Kenya. | Medmastery | Radiopaedia | Website | Twitter | LinkedIn | Scopus

MBChB (hons), BMedSci - University of Edinburgh. Living the good life in emergency medicine down under. Interested in medical imaging and physiology. Love hiking, cycling and the great outdoors.