
![]()
CXR Case 034
A 54 yo man presents hypoxaemic with worsening of a long standing productive cough and low grade fever. He stopped smoking 20 years ago.

AP CXR 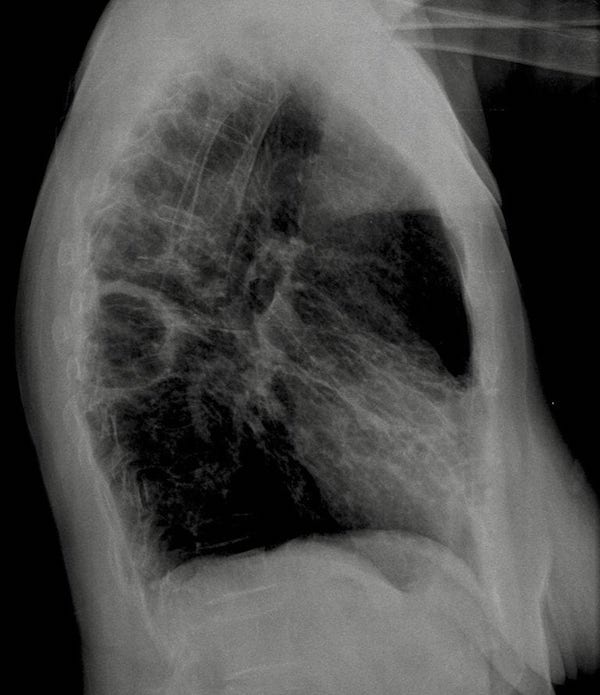
Lateral CXR
click images to enlarge
Describe and interpret this AP and Lateral CXR
CHEST X-RAY INTERPRETATION
CXR Interpretation:
This AP film has an irregular thin walled large cavity in the medial right mid zone.
The hilar vessels are visible suggesting it is situated either posteriorly or anteriorly .
There are coarse reticular markings in the right middle lobe and lingular lobes suggestive of bronchiectasis.
Lateral CXR Interpretation:
The lateral confirms the presence of a cavity in the right apical segment of the lower lobe. There is no fluid level.
The is some scattered surrounding airspace shadowing (consolidation)
CLINICAL CORRELATION
There is a single large cavity and evidence of chronic lung disease and the history suggests a more recent deterioration.
Relevant differentials include lung cancer (classically squamous cell) and infection.
A maturing pulmonary infarct from PE can cavitate.
*TB should be considered as mycobacterium are frequently found in this pattern of bronchiectasis.*
CLINICAL PEARLS
If there is a draining bronchus there won’t necessarily be a fluid level in an abscess caused by infection.
TOP 150 CXR SERIES
![]()
![]()
![]()
Prof Fraser Brims Curtin Medical School, acute and respiratory medicine specialist, immediate care in sport doc, ex-Royal Navy, academic| Top 100 CXR | Google Scholar | ICIS Course ANZ