
![]()
CXR Case 103
26 year old man. Low speed driver of motorbike vs. car.
Initial primary survey complete with soft tissue grazes on limbs only. Now increasingly agitated with falling BP.
Describe and interpret this CXR
CHEST X-RAY INTERPRETATION
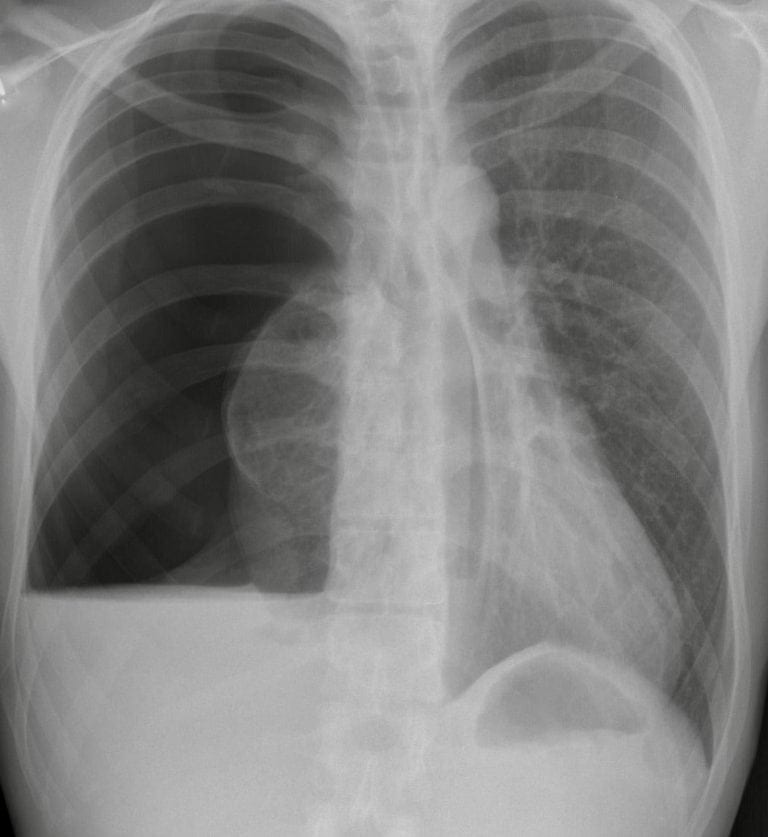
There is a right tension pneumothorax with displacement of the mediastinum to the left.
There is a right sided air fluid level suggesting haemothorax. No obvious rib or clavicular fractures.
CLINICAL CORRELATION
Tension pneumothorax
This needs immediate recognition and a needle decompression. Rapid progression to a decent size chest tube is indicated.
CLINICAL PEARLS
Hypotension in the context of trauma is hypovoloaemia from haemorrhage (somewhere) until proven otherwise. A diagnosed haemopneumothorax can contribute to hypotension in 2 ways;
- Hypovolaemic shock from the blood extravasating into the chest
- Obstructive shock from the raised intrathoracic pressure obstructing venous return
TOP 150 CXR SERIES
Prof Fraser Brims Curtin Medical School, acute and respiratory medicine specialist, immediate care in sport doc, ex-Royal Navy, academic| Top 100 CXR | Google Scholar | ICIS Course ANZ
Good case but hypovolaemia is much more common cause of hypotension in trauma than tension pneumothorax. Hypotension with tension pneumothorax is far more common in +ve pressure ventilated patients than -ve pressure spontaneously breathing patients. It can however occur in the latter when it is usually late and an indicator of imminent decompensation. Important to emphasize here that even if BP improves with Tension decompression any trauma patients (even without obvious haemothorax on CXR) are still bleeding until proven otherwise.