
![]()
ECG Case 047
Middle-aged patient presenting with palpitations. Describe the ECG
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
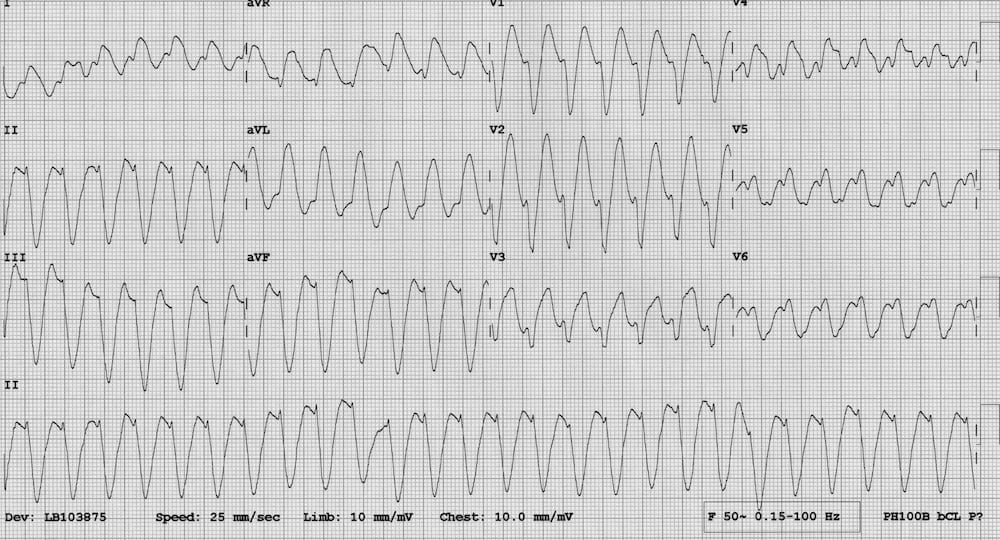
This is another example of ventricular tachycardia, this time with a dominant S wave in V1/V2 and therefore a LBBB morphology (compare this with ECG 046).
Regular broad complex tachycardia at ~ 160 bpm.
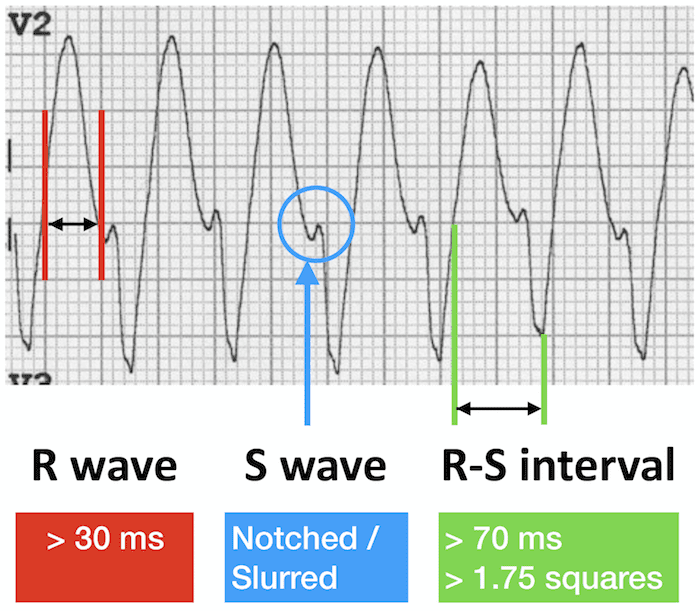
- Initial R wave > 30 ms wide, RS interval > 70 ms (Brugada sign)
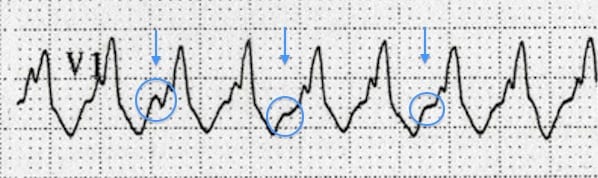
- Notching/slurring of the downslope of the S wave in V1/V2 (Josephson sign).
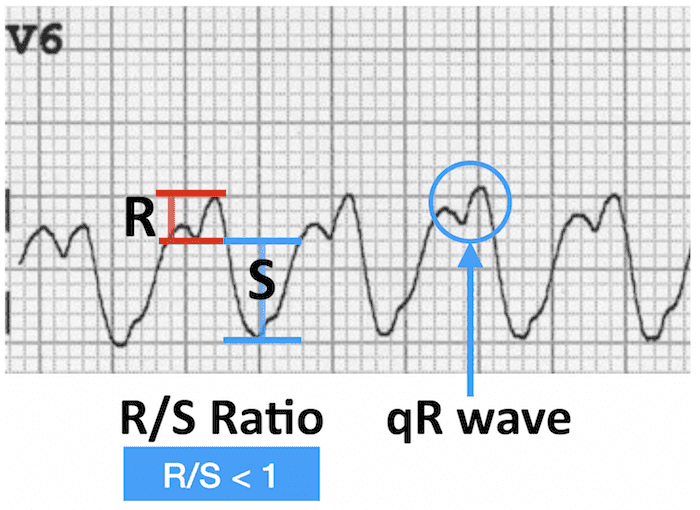
- Dominant S wave in V6; qR wave; absence of typical LBBB morphology
- Abnormal axis with positive aVR, although does not quite meet criteria for northwest axis.
NB. Note that a positive Brugada sign only requires an RS interval of >60 ms when LBBB morphology is present, compared to >100 ms when RBBB morphology is present.

Dominant S Wave in V1 or V2 (LBBB Morphology)
Lead V1 or V2
Lead V6
These features are very different to the expected pattern in LBBB, which has:
- Dominant S wave in V1, but with an R/S interval < 70 ms and minimal initial R wave.
- Dominant R wave in V6 (often slurred).

CLINICAL PEARLS
Tips for Spotting VT when LBBB morphology present
[NB. LBBB morphology = QRS > 120ms with dominant S wave in V1]
Suspect VT in any patient with a regular broad complex tachycardia (esp if > 160 ms wide).
Look at aVR
- Positive QRS complex?
- Leads I and aVF negative?
- If yes to both -> northwest axis is present -> probable VT.
Look at V1
- Initial R wave > 30 ms? –> probable VT.
- Notching of the S wave (Josephson’s sign)? –> probable VT.
- RS interval > 70 ms (Brugada’s sign)? –> probable VT.
- None of the above –> possible SVT with LBBB.
Look at V6
- Dominant S wave (R/S ratio < 1)? -> probable VT.
- Dominant R wave (R/S ratio > 1)?-> possible SVT with LBBB.
If still uncertain, scrutinise the ECG for:
- AV dissociation — P waves randomly deforming the QRS complexes and T waves.
- Fusion and capture beats.
If still uncertain…review the ECG for:
- AV dissociation — P waves randomly deforming the QRS complexes and T waves
- Fusion and capture beats.
AV dissociation: superimposed P waves at a different rate to the QRS complexes
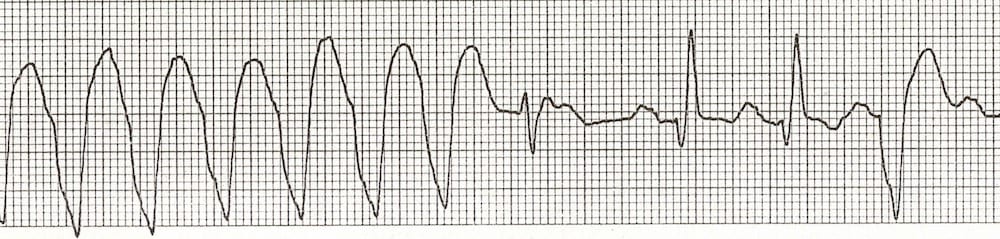
The first of the narrower complexes is a fusion beat, the next two are capture beats.
References
Further Reading
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
TOP 100 ECG Series
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |