
![]()
ECG Case 106
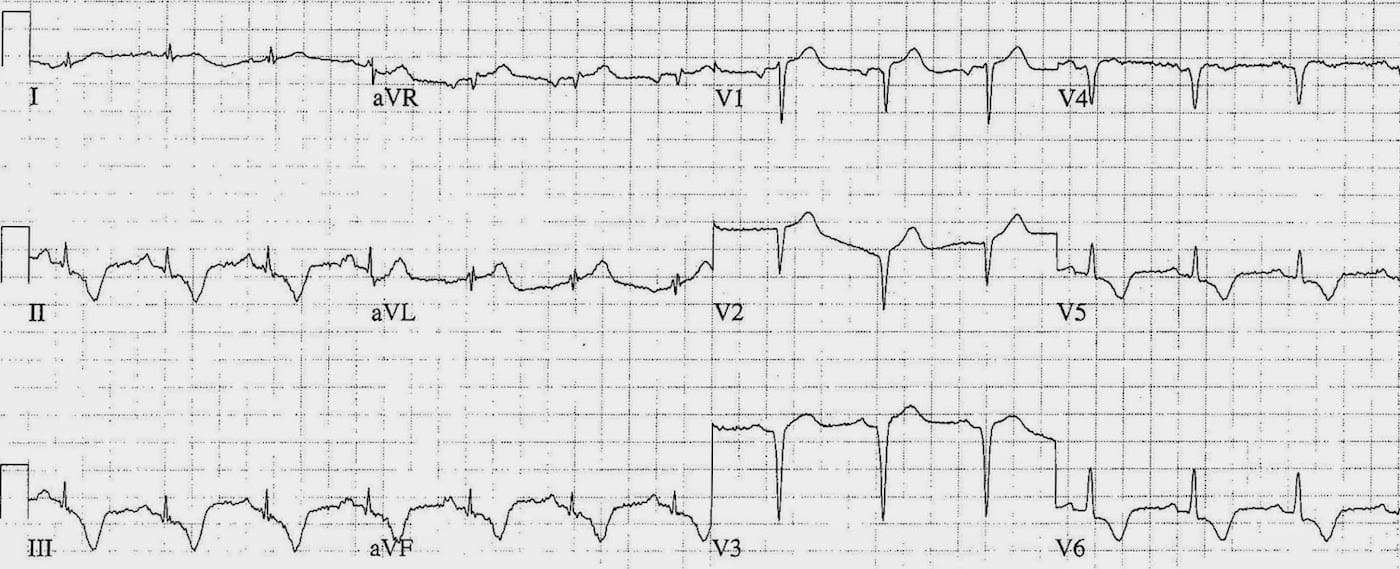
In Case 105, a 70yr old male presented with chest pain, palpitations and hypotension. He underwent DC cardioversion and this is his post cardioversion ECG.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Rate:
- 78
Rhythm:
- Regular
- Sinus rhythm
Axis:
- Normal
Intervals:
- PR – Normal (~180ms)
- QRS – Normal (100ms)
- QT – 320ms (QTc Bazett 370 ms)
Segments:
- ST Elevation leads V1 & V3 ?? aVF
- ST Depression leads II, III, aVF, V5-6
- ST segment analysis difficult due to baseline wander
Additional:
- Deep symmetrical T wave inversion leads II, III, aVF, V5-6
Interpretation:
Without more clinical information on the case including prior medical history, findings on serial ECG’s, old ECG’s, and result of further investigations post this episode e.g. echo or angio it’s difficult to give a clear conclusion to this case and ECG.
CLINICAL PEARLS
The broad differentials for the findings on this ECG are:
- Ischemia
- Structural Heart Disease
- Cardiac T-wave Memory
T wave memory is an interesting phenomenon that could explain the marked T wave changes seen on this ECG. It results in transient T wave changes following a period of abnormal ventricular conduction e.g. ventricular tachycardia, paced rhythms, intermittent bundle branch block or aberrant conduction.
Vakil et al provide a nice overview of T-wave memory, proposed mechanisms, and a case example.
The deep T wave inversion on this ECG correspond to the leads in which a negative QRS was seen in the patients pre-cardioversion ECG (Case 105) a finding consistent with T-wave memory. Patient’s often require work-up to exclude underlying ischaemia or structural disease but cardiac T-wave memory is a benign and self-resolving condition in itself.
REFERENCES
Other cases on the blog with Cardiac T-wave memory:
References on Cardiac T-wave memory
- Vakil K, Gandhi S, Abidi KS, et al. Deep T-Wave Inversions: Cardiac Ischemia or Memory? JCvD 2014;2(2):116-118
- Folco EJ, Roder K, Mitchell GF, Koren G. “Cardiac memory”: a struggle against forgetting. Circ Res. 2003 Sep 5;93(5):384-6.
- Ghosh S, Rhee EK, Avari JN, Woodard PK, Rudy Y. Cardiac Memory in WPW Patients: Noninvasive Imaging of Activation and Repolarization Before and After Catheter Ablation. Circulation. 2008 Aug 26;118(9):907-15.
- Chiale PA et al. The multiple electrocardiographic manifestations of ventricular repolarization memory. Curr Cardiol Rev. 2014 Aug;10(3):190-201.
- Ali FS, Baranchuk A. Cardiac Memory Variations in Surface ECG Precordial Mapping. The Journal of Innovations in Cardiac Rhythm Management (JICRM). 2014
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |

Interesting case. I would like to have more of the follow up. How could it be flutter with rbbb and lah since the post cardioversion ECG doesn’t show these changes? Do you think these were rate related?
Friendly
George