
![]()
ECG Case 105
ECG is from a 70yr old male who presented with chest pain and palpitations.
Vital signs: BP 85/64 RR 20 Sats 98% on 10L/min.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
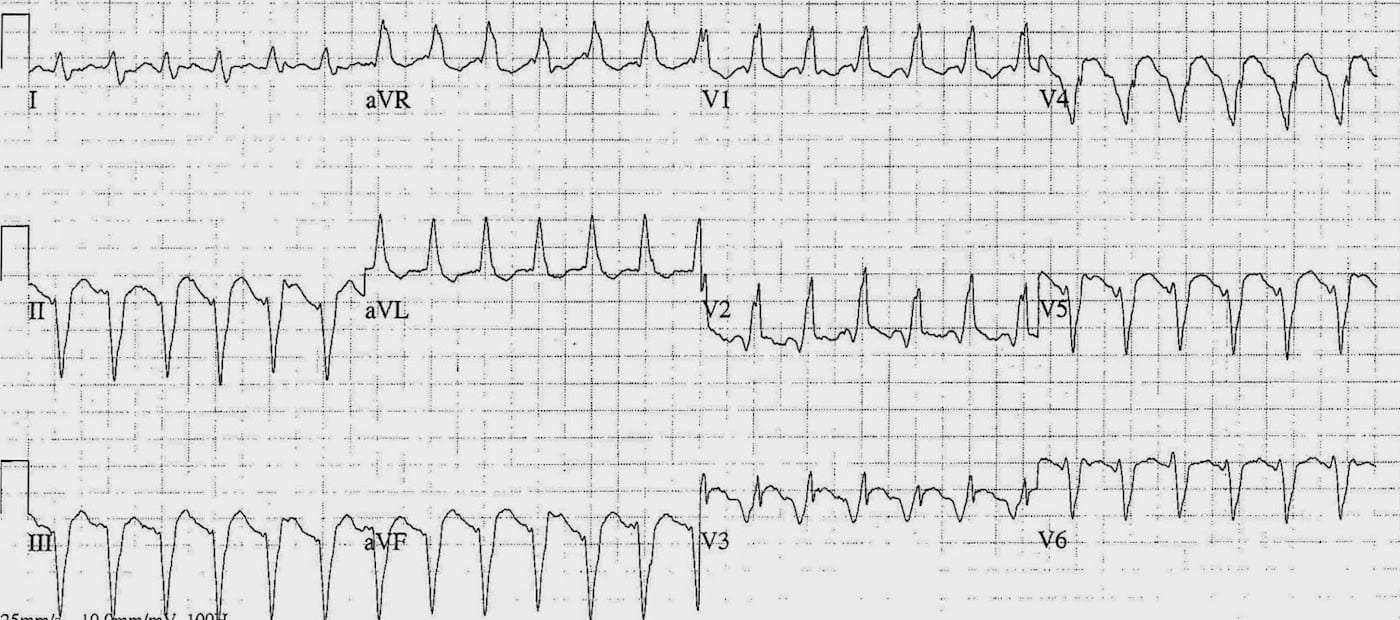
Rate:
- 150
Rhythm:
- Regular
Axis:
- LAD (~ 80deg)
Intervals:
- QRS – Prolonged (140ms)
- QT – 320ms
Additional:
- RBBB Morphology
- Typical morphology
Interpretation:
- Regular Wide Complex Tachycardia
- Clinical compromise evidence by chest pain and hypotension
CLINICAL OUTCOME
General differential diagnosis include:
- Ventricular Tachycardia
- SVT with aberrancy
- SVT with pre-existing conduction delay
- SVT with pre-excitation
- Not applicable in this case but don’t forget paced rhythms
But what about this ECG? This ECG is most probably SVT (likely atrial flutter) with RBBB aberrancy as the principle diagnosis. The QRS activation pattern of rapid activation till QRS peak followed by slower activation is classic for RBBB aberrancy.
The combination of RBBB and LAD (left axis deviation) means the SVT exit is the left posterior fascicle (left mid to basal LV), if this was VT it would be a fascicular VT.
Check out the links below for more on VT vs SVT with aberrancy and also on fascicular VT:
- ECG Library – Ventricular Tachycardia
- ECG Library – VT vs SVT with aberrancy
- ECG Library – Fascicular VT
What happened next?
…the patient underwent DC cardioversion in the Emergency Department and his post cardioversion ECG can be interpreted as Top 100 ECG Case 106
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |
I don’t understand how this is likely SVT – A-flutter. in all of the lateral leads, the deflection is negative, making it, to me, appear to be of ventricular origin. I am 0 for 50 on these things, and when I show these to any cardiologist, I get nothing but different answers between all of them.
The rate of 150 is common in A. Flutter 2:1 Conduction I think.
I would have thought it was VTach at first glance but im just a humble ambo tech and im sure John knows better!!!
Am I crazy, or are those p waves?
I too saw regular P waves with atrial ~80-90. would think this is VT with AV dissociation
left posterior fascicular VT, How can it b svt with R/s < 1 IN V6
I don’t understand how there is a RBBB if there is a LAD?
Why don’t look at those p waves that is seen obvious in lead 2 with embeded p waves in the T waves that made AV dissociation,
and what about the left rabbit ear in V1 ,
what about positive brugada sign since from R wave to nadir of S wave in lead V 5 or V6 is at least of about 100 ms or more ,
what about the old age and the chest pain of this patient !!!
after all that you said it is atrial flutter!!!!