
![]()
ECG Case 117
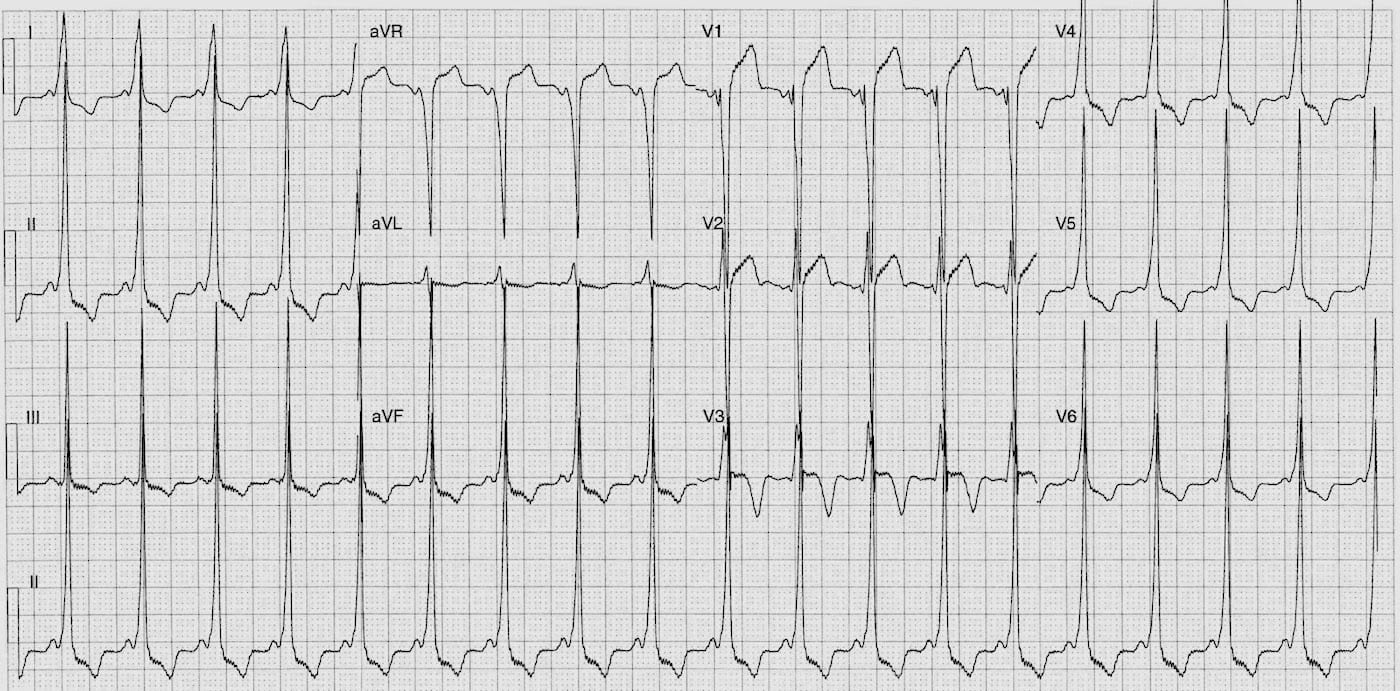
ECG of a 14yr old female who presents following an episode of palpitations and associated dizziness.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Rate:
- 110-115 bpm
Rhythm:
- Regular
- Sinus rhythm
Axis:
- Normal
Intervals:
- PR – Short (80ms)
- QRS – Prolonged (120ms)
- QT – 340ms (QTc Bazett 460 ms)
Segments:
- ST Elevation leads aVR, V1-2
- ST Depression leads I, II, III, aVF, V4-6
Additional:
- Delta waves best seen inferolaterally
- T wave inversion leads I, II, III, aVF, V3-6
- ‘Pseudo’ left ventricular hypertrophy
- Prominent R waves leads I, II, III, aVF, V4-6
- Deep S waves leads aVR, aVL, V1-2
Interpretation:
- Wolff-Parkinson-White syndrome
- Right anteroseptal pathway – using Arruda algorithm
- Voltage & ST/T changes secondary to pre-excitation
- Patient requires referral for an EP study.
FURTHER DISCUSSION
The right anteroseptal pathway can be difficult to ablate due to the close proximity of the AV node and risk of AV nodal injury during ablation.
Cryothermal ablation and careful mapping may be required rather than RF ablation. A more detailed review of septal accessory pathways and ablation techniques can be found here:
- Macedo PG, Patel SM, Bisco SE,Asirvatham SJ. Septal Accessory Pathway: Anatomy, Causes for Difficulty, and an Approach to Ablation. Indian Pacing Electrophysiol J. 2010; 10(7): 292-309.
There are two commonly used algorithms to identify accessory pathway location from the surface ECG, the Arruda algorithm and Milstein algorithm. You can also download a free app called EP Mobile which incorporates both algorithm’s in addition to lots of other useful EP formulas (iTunes or Google play)
Arruda algorithm
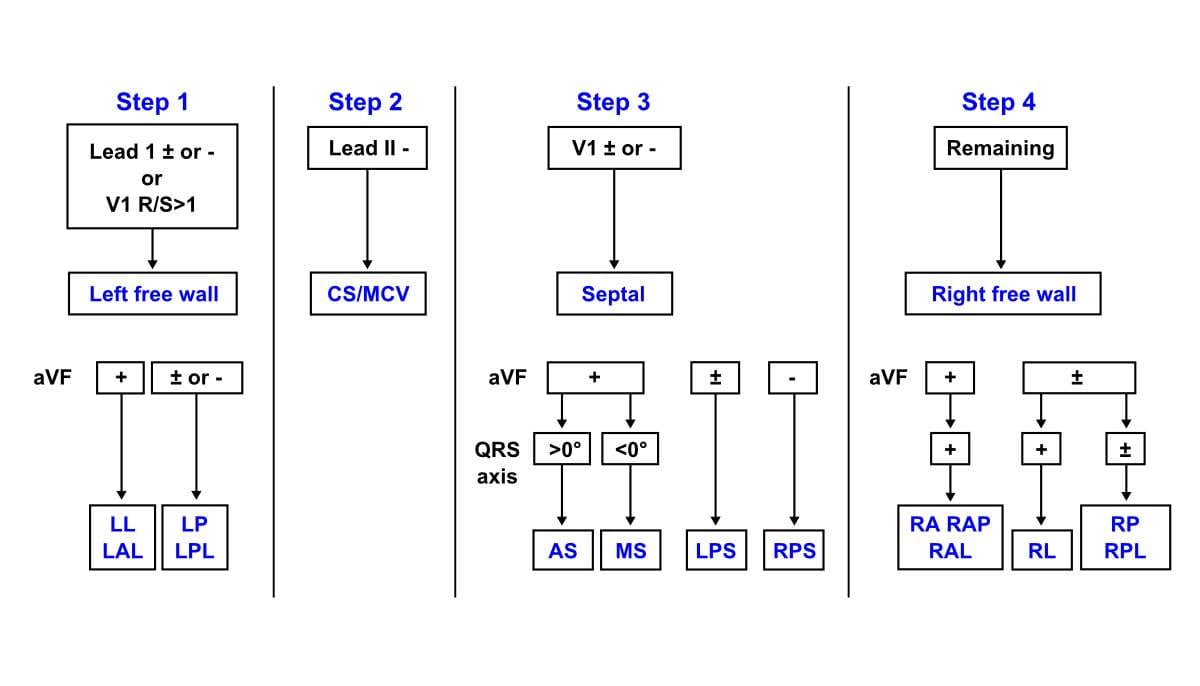
Arruda MS et al. Development and validation of an ECG algorithm for identifying accessory pathway ablation site in Wolff-Parkinson-White syndrome. J Cardiovasc Electrophysiol. 1998 Jan;9(1):2-12.
Milstein algorithm

Milstein S et al. An algorithm for the electrocardiographic localization of accessory pathways in the Wolff-Parkinson-White syndrome. Pacing Clin Electrophysiol. 1987 May;10(3 Pt 1):555-63
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |

Question about ECG case 117. Somehow I initially missed the WPW and called it a LBBB with positive Scarbossa in V3. Can WPW and a LBBB exist together? If so, does Scarbossa’s criteria still apply?
Thank you for these ECGs, they’re truly making me better.