
![]()
ECG Case 118
This ECG is from a 35 yr old male Type 1 diabetic. He presents feeling generally unwell with abdominal pain and dyspnea.
Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
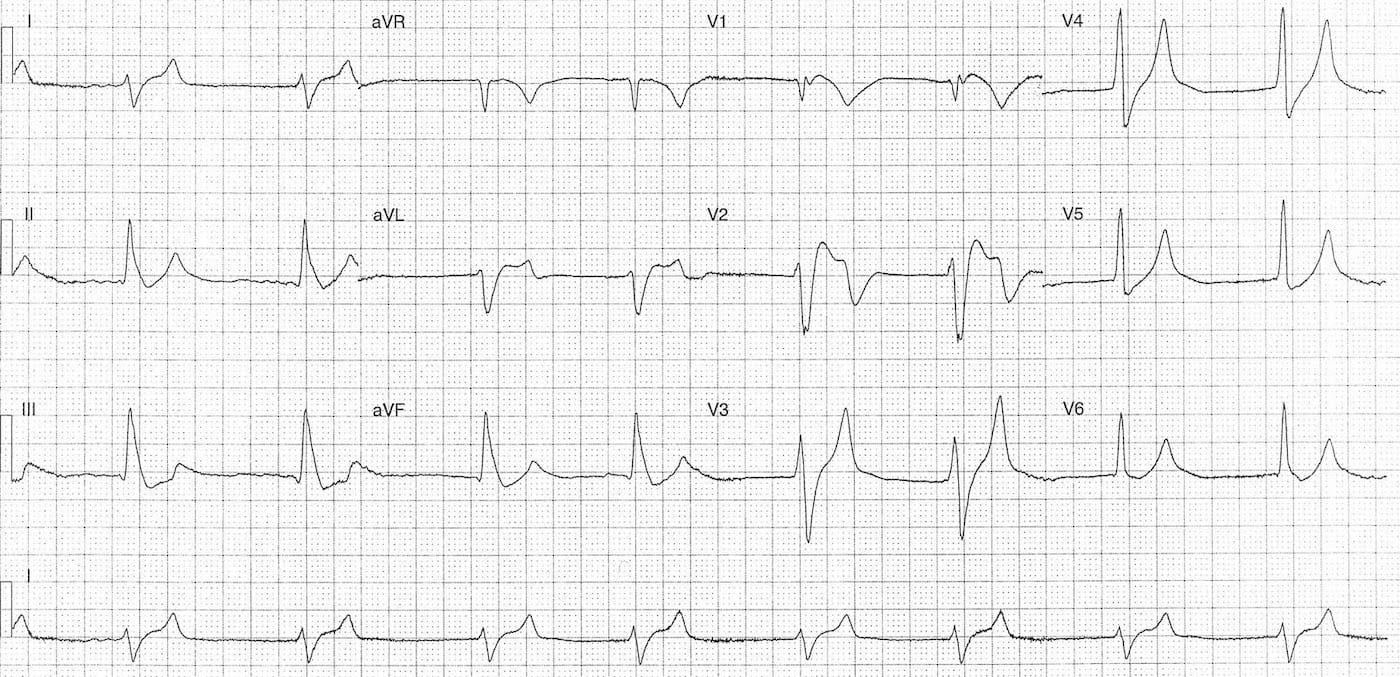
Rate:
- 48 bpm
Rhythm:
- Irregular
- Nil P waves visible
Axis:
- Right axis deviation
Intervals:
- QRS – Prolonged
Additional:
- ST Elevation leads I, aVL, V1-4
- ST depression leads III, aVF
- Bizarre broad QRS without typical BBB
- Prominent T waves leads V3-6
Key abnormalities:
- Slow atrial fibrillation
- QRS Prolongation
- High lateral ST elevation
- Prominent precordial T waves
The differentials of these ECG findings are relatively broad but the immediate life-threats would be:
- Acute myocardial infarction
- Hyperkalaemia +/- acidaemia
- Drug toxicity
Other causes include myocarditis, cardiomyopathy and hypothermia.
CLINICAL OUTCOME
We must always take our ECG differentials to the bedside and consider them within the clinical presentation and scenario. ECG abnormalities in the acutely unwell diabetic should always prompt consideration of hyperkalaemia and acid-base disturbance as the primary cause. We must also be mindful that diabetic emergencies can be precipitated by acute cardiac ischaemia and also cause hypercoagulable states.
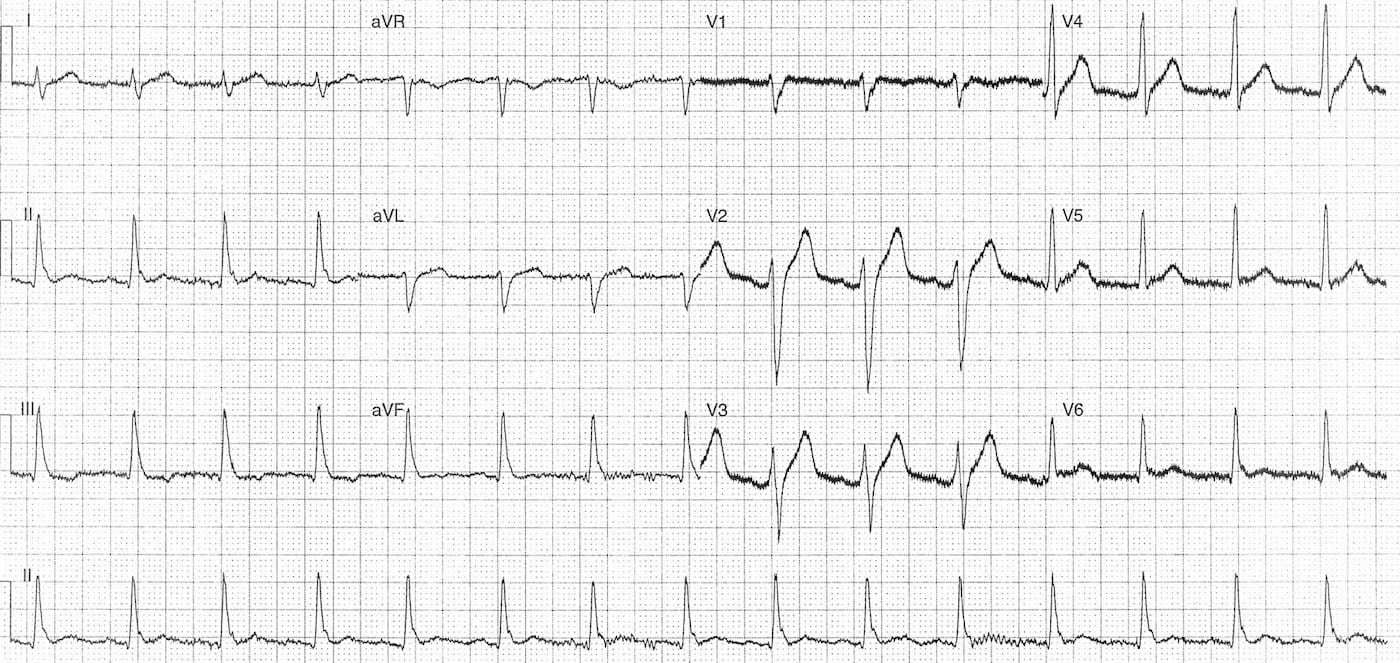
This patient had no associated chest pain nor any history of cardiac disease. The patients initial VBG showed diabetic ketoacidosis with severe hyperkalaemia, K 8.7 mmol/L. Following initial treatment of DKA and hyperkalaemia a repeat ECG was performed with K 5.4 mmol/L.
We can now see resolution of the QRS prolongation, restoration of sinus rhythm and normalisation of the ST / T wave changes.
TOP 150 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |
Fibrillatory waves and No “P” wave suggestive of Atrial Fibrillation.
More than likely sinus arrest with junctional escape vs AF. Looks most like mild musculoskeletal baseline artifact in ECG 1.
1.AF or escape – junctional/ventricular – rhythm? Rather AF but nobody can be sure
2. After stabilization I’d suggest a coronary angiography because he is a young diabetic man and these ECG changes are somewhat ischemic.
Very nice case, thank you
Lead I looks like A-Fib. Accelerated Idioventricular rhythm with ST elevations in V2, V3 and reciprocal depressions in leads II and AVF suggesting septal/anterior MI. Tall narrow T waves in precordials V3-V6 – you would want to R/O hyperkalemia
Interesting case. Junctional rhythm ± AF. Underlying CAD cannot be ruled out but changes do normalize after hyperkalemia correction. Possible indication for elective ischemia testing, especially if positive troponin.
Agree. QRS duration normalized in ECG 2. T wave also indicating correction of hyperkalemia (which was confirmed initially). The ventricular waves are not much irregular (slightly so due maybe to resp cycle) – ?? Junctinal rhythm. The ST elevation on ECG 1 should be of consideration (possible MI) – author revealed that pt did not have chest pain. A lipid panel shoyld be done