
![]()
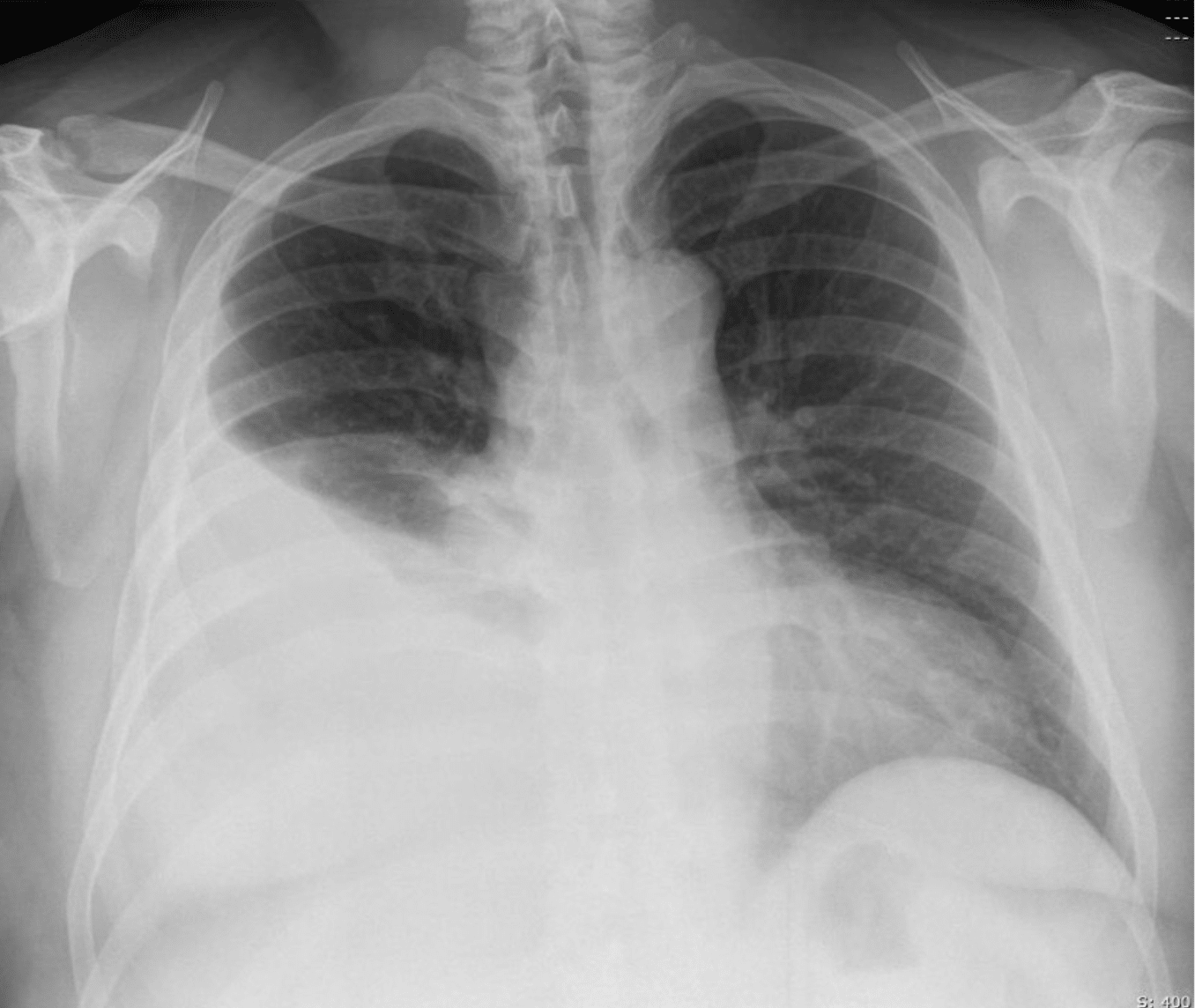
FFS: Pleural Effusion
Pleural effusion is the accumulation of fluid in the pleural space. Diagnosis is usually clinical and confirmed on CXR, though ultrasound or CT may be required. Pleural aspiration may be needed for diagnosis or to relieve dyspnoea.
Pathology
Pleural effusions are classified as transudates or exudates, though the distinction is not always clear-cut.
Transudates
- CCF
- Hypoalbuminaemia
- Hypothyroidism
- Meigs syndrome
Exudates
- Infection (including TB)
- Malignancy
- Connective tissue disease
- Subdiaphragmatic (e.g. subphrenic abscess, pancreatitis)
- Irradiation
- Trauma
Clinical Assessment
History
- Degree of dyspnoea
- Cough, haemoptysis
- Orthopnoea, exertional dyspnoea (CCF)
- Risk factors: malignancy, asbestos, TB
- History of trauma
- Medications, especially anticoagulants
Examination
- Vital signs and pulse oximetry
- On affected side:
- ↓ Breath sounds
- ↓ Vocal resonance
- Dull percussion note
Investigations
Bloods
- FBC
- CRP
- U&Es, glucose
- Coagulation profile
- ABGs
Imaging
- CXR: primary investigation for effusion
- Ultrasound: confirms effusion, guides aspiration
- CT chest: useful if malignancy, consolidation, or loculation suspected
Pleural Aspiration
Once aspirated, pleural fluid is sent for analysis of the following:
- M&C (incl. AFB stain)
- Cell counts (RBCs, neutrophils, lymphocytes)
- Cytology
- Biochemistry:
- Protein & LDH to classify transudate vs exudate
- pH: <7.2 suggests infection
- Glucose: ↓ in infection, RA
- Rheumatoid factor
- Triglycerides (chylothorax)
Transudate vs Exudate
Light’s Criteria can be used to differentiate transudates from exudates.
| Test | Exudate | Transudate |
|---|---|---|
| Protein | >30 g/L | <30 g/L |
| LDH | >200 IU/L | <200 IU/L |
| Pleural:serum protein ratio | >0.5 | <0.5 |
| Pleural:serum LDH ratio | >0.6 | <0.6 |
Management
- Pleural tap
- Indicated for dyspnoea or diagnosis
- Large effusions may require drainage
- Refer to radiology for ultrasound-guided tap if small or loculated
- Treat underlying cause
- Pleurodesis
- For recurrent symptomatic effusions
- Particularly useful in malignancy
Appendix 1
References
FOAMed
- Nickson C. Pleural Effusion. CCC
- Rippey J. Lung ultrasound: Pleural effusion. LITFL
- Rippey J. Pleural Effusion Case 001. LITFL
- Rippey J. Pleural Effusion Case 002. LITFL
- Rippey J. Ultrasound Case 025. LITFL
- Brims F. CXR Case 096. LITFL
- Tylee T. Hypothyroidism. MedMastery
- Cadogan M. Pleural Fluid Analysis. LITFL
- Cadogan M. Pleural Tap. LITFL
Resources
- Rea H, McAuley S, Jayaram L, Garrett J, Hockey H, Storey L, O’Donnell G, Haru L, Payton M, O’Donnell K. The clinical utility of long-term humidification therapy in chronic airway disease. Respir Med. 2010 Apr;104(4):525-33.
- Helviz Y, Einav S. A Systematic Review of the High-flow Nasal Cannula for Adult Patients. Crit Care 2018; 22: 71
- Parke RL, Bloch A, McGuinness SP. Effect of Very-High-Flow Nasal Therapy on Airway Pressure and End-Expiratory Lung Impedance in Healthy Volunteers. Respir Care. 2015 Oct;60(10):1397-403
- Li J, Albuainain FA, Tan W, Scott JB, Roca O, Mauri T. The effects of flow settings during high-flow nasal cannula support for adult subjects: a systematic review. Crit Care. 2023 Feb 28;27(1):78.
Fellowship Notes

BA, BM BCh University of Oxford, PgCert (Medical Education)University of Dundee. Aspiring medical physician with a particular interest in respiratory medicine, public health and medical education

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |