
![]()
Jacques Calvé

Jacques Calvé (1875-1954) was a French orthopaedic surgeon.
Calvé was a French orthopaedic surgeon whose name endures as maladie de Calvé (Legg-Calvé-Perthes disease) and several other musculoskeletal eponyms. Trained in Paris under Albert Calmette and working in the shadow of Koch’s discoveries, Calvé established himself as a meticulous observer of bone and joint pathology, particularly tuberculosis of the spine and hip. His clinical acumen and willingness to apply new radiographic techniques positioned him at the forefront of early 20th-century orthopaedics.
In 1910, Calvé independently published his account of childhood hip necrosis, contemporaneous with Legg in Boston and Perthes in Tübingen. Rejecting the prevailing idea of tuberculous coxitis, he argued instead for a vascular cause of epiphyseal collapse, recognising the non-infective nature of the disorder. His broader interests extended to Pott paraplegia, scoliosis, spinal deformity, and vertebral osteochondritis, where his writings clarified diagnostic criteria and guided treatment at a time when modern orthopaedic surgery was in its infancy.
Calvé combined surgical practice with an enduring dedication to teaching and research. His writings included practical guides on plaster techniques, methods to manage tuberculous abscesses, and detailed descriptions of vertebral collapse now known as Calvé disease (vertebra plana). By the time of his death in 1954, he was regarded as one of France’s leading orthopaedic voices, and his legacy remains fixed through the enduring eponyms that continue to mark paediatric orthopaedics and spinal pathology.
Biography
- Born on August 18, 1875 in Paris, France.
- 1902–1906 – Intern in Paris hospitals; completes doctoral thesis in 1906: De la Coxalgie double chez l’enfant.
- 1906–1920 – Assistant surgeon at the Hôpital Maritime, Berck-sur-Mer, under Maxime Ménard. Focused on musculoskeletal tuberculosis.
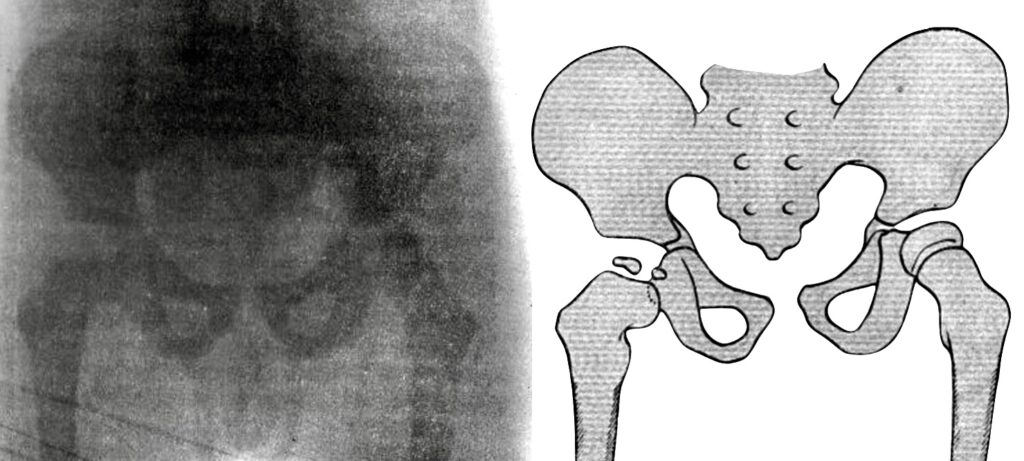
- 1910 – Publishes Pseudo-coxalgie based on radiographs of 500 children with hip tuberculosis, identifying 10 cases of a distinct, non-tuberculous hip disorder. Later termed Legg–Calvé–Perthes disease (LCPD).
- 1917 – With Marcel Galland, publishes Les appareils platrés and describes novel treatment of Pott’s paraplegia by aspiration of abscesses.
- 1920 – Adopts Waldenström’s term Coxa plana for the condition previously termed “pseudo-coxalgie.”
- 1925 – Describes vertebral osteochondritis, later termed Calvé’s disease (vertebra plana).
- 1925 – Becomes chief surgeon at Berck after Ménard’s retirement. With American support, establishes La Fondation Franco-Américaine de Berck, an orthopaedic hospital and trade school.
- 1931 – Publishes Le traitement de la tuberculose osseuse, summarising his experience with skeletal tuberculosis.
- 1937 – Reflects on LCPD as a still “mysterious” disorder, describing five key pathological features.
- World War II – Hospital at Berck bombed; Calvé evacuates patients to the Hôpital Dominique Larrey in Versailles.
- 1945 – Retires from Berck; moves to the United States for four years, welcomed by American orthopaedic colleagues.
- 1953 – Returns to Berck, health declining.
- Died March 10, 1954 in Berck-sur-Mer at age 79.
Medical Eponyms
Legg-Calvé-Perthes disease (LCPD); (1910)
Legg–Calvé–Perthes disease (LCPD) is a childhood hip disorder caused by avascular necrosis of the proximal femoral epiphysis, leading to progressive collapse and deformity of the femoral head. It typically presents between ages 4–10, with insidious hip pain, limp, and reduced range of motion.
In 1910, Legg, Calvé and Perthes independently reported a hip disease in children with a symptomatic picture resembling that described by Henning Waldenström in 1909. These authors believed the process to be unrelated to tuberculosis:
Calvé published a detailed account of the disease process highlighting the non-tuberculous nature of the condition and linked it to vascular insufficiency of the femoral head rather than infection or trauma. Calvé described affected children with limping gait, stiffness, and characteristic radiographic changes of the femoral head, summarising:
Original
English
En résumé, tous ces cas se ramènent à une arthrite transitoire, de durée courte, se développant sur des sujets porteurs de déformations de l’extrémité supérieure du fémur: coxa vara, hypertrophie de la tête fémorale, atrophie lamellaire du noyeau osseux de l’épiphyse, avec conservation des rapports normaux de surfaces articulaires. Comment faut-il interpréter des lésions osseuses?
Il est naturel, dès qu’il s’agit d’une arthrite chronique de la hanche, de songer à une coxo-tuberculose… A notre avis , ce diagnostic nous parait erroné et nous le rejetons pour plusieurs raisons…
Nous nous trouvons, en effet, en présence d’une ostéogenèse anormale et retardée, ce qui parait plutôt être du ressort du rachitisme. Sans avoir la présomption de conclure, nous avouerons que, jusqu’à plus ample informé, cette solution nous semble la plus plausible.
In summary, all the cases point to a transitory arthritis, of short duration, which develops in those who carry a deformity of the upper extremity of the femur: coxa vara, hypertrophy of the femoral head, atrophy of the lamellar bony nucleus of the epiphysis, with conservation of the normal relations of the articular surfaces. How must one interpret these bony lesions?
It is natural, as soon as one speaks of a chronic arthritis of the hip, to think of a coxo-tuberculosis… In our opinion, this diagnosis seems erroneous, and we reject it for several reasons…
For we are presented with an abnormal and retarded osteogenesis, which appears rather to be the consequence of rickets. Without making the presumption to conclude, we must admit that until we are more informed, this solution seems to us the most plausible.
Calvé’s Operation (1917)
Calvé’s operation is a surgical technique devised for the management of cold abscesses secondary to Pott’s disease (tuberculous spondylitis). The method involves aspiration of the abscess contents with a trocar and cannula, combined with instillation of antiseptic agents. Crucially, Calvé emphasized performing the procedure in a way that would avoid creating an external fistula or sinus tract, which could perpetuate chronic infection.
1917 – Calvé and Galland published Les appareils plâtrés describing their approach as a safer alternative to incision and drainage. By using aspiration rather than open surgery, he sought to minimise contamination and improve healing in patients already debilitated by spinal tuberculosis. He explained that:
“L’opération consiste à ponctionner l’abcès froid avec un trocart, à en aspirer le contenu, puis à injecter une solution antiseptique, sans laisser de trajet fistuleux.”
Calvé and Galland, 1917
(“The operation consists of puncturing the cold abscess with a trocar, aspirating its contents, and then injecting an antiseptic solution, without leaving a fistulous tract.”)
Calvé’s method was widely adopted in Europe during the early 20th century and became part of the conservative surgical armamentarium for tuberculous abscesses until the advent of effective chemotherapy. Today, the principle of percutaneous aspiration and drainage, rather than open incision, is still employed in selected cases, often with image guidance and antibiotics.
Calvé disease (1925) [vertebra plana]
Vertebra plana is a rare pediatric spinal disorder, typically presenting between ages 6 and 12 with thoracolumbar pain, short-segment kyphosis, and radiological flattening of a vertebral body. Today it is understood to most often result from eosinophilic granuloma (part of Langerhans cell histiocytosis), though other causes including osteochondritis, infection, or malignancy have been recorded.
1925 – Calvé described the case of a 7-year-old patient with ‘osteochondritis‘ of a vertebral body stating the condition was ‘to the spinal column what coxa plana is to the hip, and what Koehler’s disease is to the foot‘. He characterised the criteria for the disease:
- total collapse of a single vertebra,
- sparing of the intervertebral disc,
- relative widening of the adjacent intervertebral space, and
- increased density of the collapsed vertebra.
In 1927, Buchman proposed the name vertebra plana for the condition. By the 1950s, biopsy studies (Compere, 1954) showed many cases were due to eosinophilic granuloma, not osteochondritis, and the debate on aetiology continues. Today, the term vertebra plana describes the radiological finding, while Calvé’s disease is usually reserved for rare cases of true osteochondritis of a vertebral body.
Major Publications
- Calvé J. De la Coxalgie double chez l’enfant. Th. Méd. Paris, 1905
- Calvé J. Sur une forme particulière de pseudo-coxalgie greffée sur des déformations caractéristiques de l’extrémité supérieure du fémur. Revue de chirurgie 1910; 42: 54–84 [Clin Orthop Relat Res. 1980; 150: 4-7. PMID 7000409]
- Calvé J. The Importance of Maritime Hospitals in the Treatment of Surgical Tuberculosis. 1913
- Osgood RB, Calvé J. Certains types d’arthrite déformante et leur traitement. 1914
- Calvé J, Galland M. Les appareils platrés. 1917
- Calvé J. Sur un nouveau traitement des paraplégies pottiques. 1918
- Calvé J. A localized affection of the spine suggesting osteochondritis of the vertebral body, with the clinical aspects of Pott’s disease. The Journal of Bone & Joint Surgery 1925; 7(1): 41–49.
- Calvé J, Galland M, Mozer MC. La tubercolose ostéo-articulaire : évolution, diagnostic de début et traitement. 1935
- Calvé J, Galland M, de Cagny R. Pathogenesis of the limp due to coxalgia. The Journal of Bone & Joint Surgery 1939; 21(1): 12
- Calvé J. Die Knochen- und Gelenktuberkulose; Verlauf, Frühdiagnose und Behandlung. 1946
References
Biography
- HP. Jacques Calvé. The Journal of Bone and Joint Surgery. 1954; 36B: 503-504
- Compere EL, Johnson WE, Coventry MB. Vertebra plana (Calvé’s disease) due to eosinophilic granuloma. J Bone Joint Surg Am. 1954 Oct;36-A(5):969-80.
- Schulitz KP, Dustmann HO. Jacques Calvé (1875-1954). In: Morbus Perthes: Ätiopathogenese, Differentialdiagnose, Therapie und Prognose. Springer. 1991: 10-13
- Schulitz KP, Niggemeyer O. Jacques Calvé. Spine (Phila Pa 1976). 1996; 21(7): 886-890.
- Beighton P, Beighton G. Calvé Jaques. The Person Behind the Syndrome. Springer 1997: 38-39
- Mostofi SB. Jacques Calvé. Who’s Who in Orthopedics. Springer; 2005: 51
- Bibliography. Calvé, Jacques. WorldCat Identities
Eponymous terms
- Buchman J. Osteochondritis of the vertebral body. J Bone Joint Surg (Am) 1927; 9(1): 55–66.
- Agrawal V, Patgaonkar PR, Nagariya SP. Tuberculosis of spine. J Craniovertebr Junction Spine. 2010; 1(2): 74-85
- Shisha T, Kiss S, Varga PP, Bucsi L, Pap K, Szoke G. Osteochondritis (Calvé’s disease) of a vertebral body–a rare form of vertebra plana. Eur Spine J. 2006; 15(3): 377-383
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |