
![]()
Perimortem Caesarean section
Resuscitative Hysterotomy / Perimortem Caesarean Section
Rationale
- Primarily, may increase chances of maternal ROSC as it improves maternal cardiac output ~25% by two mechanisms
- Reduces uterine blood flow
- Relieves diaphragmatic pressure and aortocaval compression
- Secondarily, may save a viable foetus
Indication
- Maternal arrest within 4 minutes (Do not wait for seniors or USS or sterile prep!)
- AND
- >24/40 gestation (Alternatively use fundal height above umbilicus or “visibly pregnant” as a good rough guide)
Contraindications
- None absolute; this is a heroic attempt in an arrested patient
Preparation
- Patient: Continue resuscitation with pregnancy modifications
- Area: The resuscitation room. There is no time for change of location.
- Equipment:
- Large scalpel e.g. 10-blade
- Retractors if available
- Bandage scissors
- Drugs: None essential but oxytocics useful besides standard resuscitation drugs.
- Staff:
- Most experienced doctor should perform procedure, ideally obstetrician but do not wait for his/her arrival
- Neonatologist and dedicated neonatal resuscitation team ideal
Procedure
- Duration should not exceed 5 minutes!
- Incise from pubic symphysis to at least umbilicus with a large scalpel along linea nigra into peritoneal cavity. Layers: skin, subcutaneous tissue, fascia between the rectus muscles, peritoneum.
- Retract abdominal wall laterally
- Reflect bladder inferiorly and empty by aspiration
- Make a small incision (~5cm) vertically into the inferior presenting part of the uterus until amniotic fluid comes or through endometrium
- Insert 2 fingers and lift up uterus from foetus
- Extend uterine incision up to fundus with safety scissors curved away from foetus
- Deliver the foetus. May need to disengage the presenting part from the pelvis.
- Clamp the cord twice and cut between clamps
- Give the neonate to the neonatal resuscitation team
Post Procedural care
- Deliver the placenta
- Swab the endometrial cavity to ensure no residual products of conception
- Pack the uterus and abdomen +/- clamp bleeding vessels and suture uterine incision
- Give synthetic oxytocin 5 units IV
- Continue maternal resuscitation
- If ROSC: watch for bleeding, consider further oxytocic drugs, TXA, antibiotic prophylaxis
- Resuscitate neonate
Complications
- Bleeding; marked with ROSC
Helpful tips
- The most difficult step is the decision to perform the procedure. Knowing the indications clearly will help to overcome any hesitation at the critical moment.
- Time is critical. Begin within 4 minutes of maternal arrest and take no longer than 5 minutes to perform the procedure. There is benefit after these time windows, but survival drops precipitously.
- Continue CPR with manual uterine displacement or left lateral tilt during and after the procedure
- Continue ventilating the patient, accounting for diaphragmatic splinting by the gravid uterus
Factors affecting foetal survival
- Time to delivery. Especially poor after 20 minutes.
- Quality of CPR
- Maturity
- NICU availability
- Pre-arrest maternal condition e.g. shocked for hours prior to arrest, chronic illness
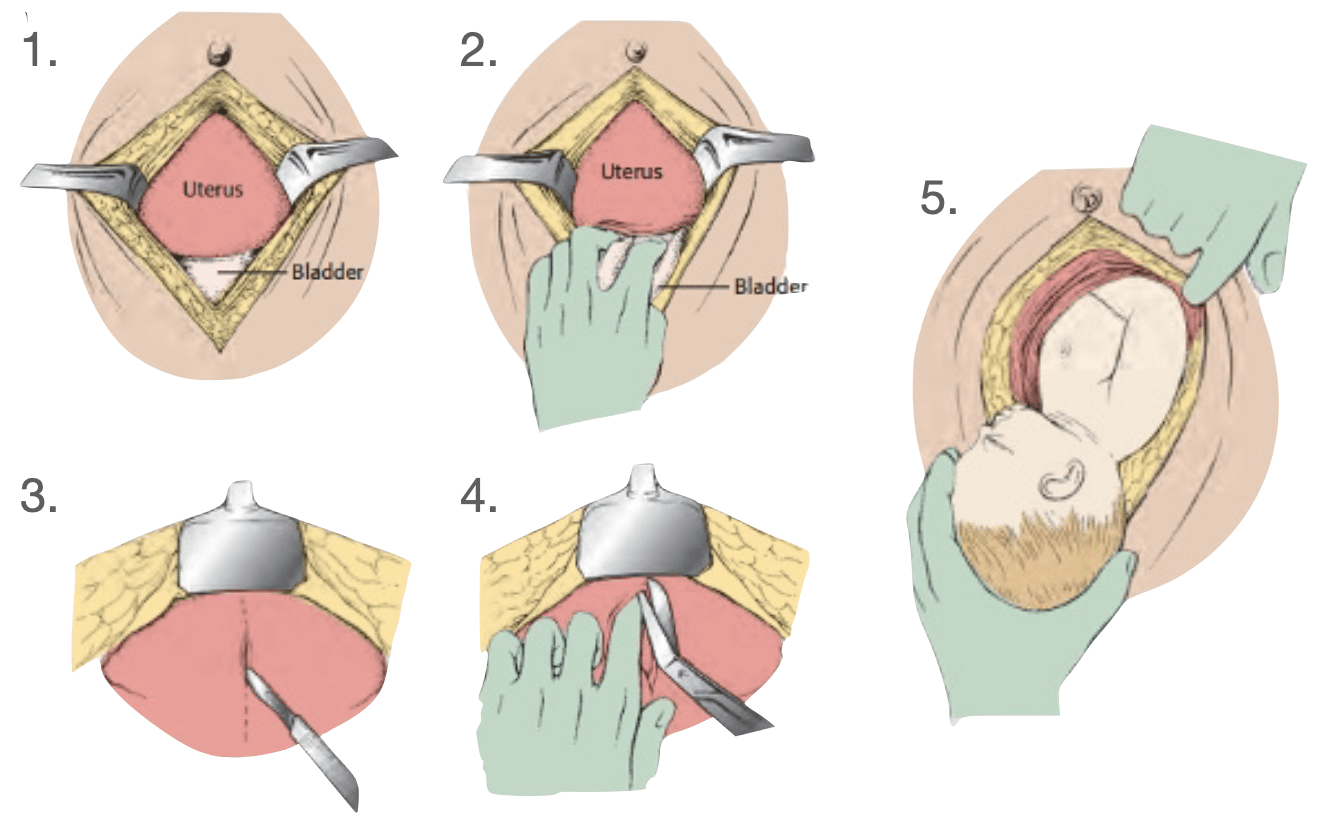
(2) Use retractors (if available) to expose the anterior surface of the uterus; Retract the bladder inferiorly.
(3) Use scalpel to make incision through the lower uterine segment.
(4) Extension of the incision superiorly using bandage scissors.
(5) Delivery of the fetus; suction the nose and mouth; clamp and cut the cord
Healy et al 2016
Further reading
FOAM
- Nickson C. CPR and Pregnancy. CCC
- Nickson C. Newborn Resuscitation. CCC
- Nickson C. Physiology of Pregnancy. CCC
- Simulation: Resuscitative Hysterotomy. SMACC
- EMCrit Conference Blast Winner: Peri-Mortem C-Section
- Perimortem C-section at St.Emlyn’s
Journal articles
- Bloomer R, Reid C, Wheatley R. Prehospital resuscitative hysterotomy. Eur J Emerg Med. 2011 Aug;18(4):241-2.
- Healy ME, Kozubal DE, Horn AE, Vilke GM, Chan TC, Ufberg JW. Care of the Critically Ill Pregnant Patient and Perimortem Cesarean Delivery in the Emergency Department. J Emerg Med. 2016 Aug;51(2):172-7.

Critical Care
Compendium

WA emergency doctor
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
[…] https://litfl.com/perimortem-caesarean-section/ […]
Hey, great resource,
I just wanted to hilight some concerns about using the 4/5 min rule as an ‘indication’.
Understood, lowest arrest to interval time is essential, however, there is evidence of survival with extended resuscitation: Maternal = 29 minutes and Neonatal = 47 minutes (Leech et al, 2024).
In a presentation by Dr Sarah Gray (subject matter expert) did a presentation at SMACC in Dublin and stated that the ‘4minute to decide and 5 minute to deliver’ rule came from 60’s and 70’s case data. We have new data that extends that timeline out significantly.
It should be changed to “as soon as possible”, it will avoid people either not transporting, or not doing the procedure if the timeframe is >5min.
https://youtu.be/L29O8E9IUAI?si=i5Mc2xvqYsQaoLf_
[…] https://litfl.com/perimortem-caesarean-section/ […]