![]()

Airway Assistant
Description of the airway assistant role in the ANZ critical care setting, including responsibilities, tips and pitfalls for newcomers to the role.

![]()
Description of the airway assistant role in the ANZ critical care setting, including responsibilities, tips and pitfalls for newcomers to the role.

Dr Laura Duggan discusses recent research quantifying airborne particle exposure when using aerosol containment devices for intubation.
Introduction to a series of posts titled "COVID-19: Keeping the baby in the bath", focusing on the need to build on existing knowledge in critical care and the appropriate testing of new therapies and innovations.
Discussing "silent hypoxaemia" and timing of intubation. Part 2 of the COVID-19: keeping the baby in the bath" series
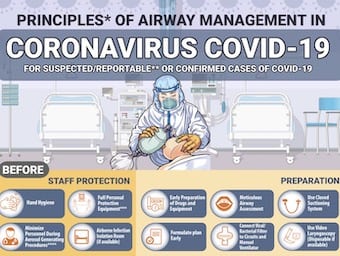
5-step COVID - a cognitive aid for the pandemic airway emphasising key consideration in the intubation of COVID19 patients.
Dr Albert Chan shares his findings from simulation testing of the "aerosol box" for the intubation of COVID-19 patients.
Today I had the opportunity to review a very nicely created Peri-intubation Action Card that was put together in short order by two anesthesiologists from Scope Anesthesia - Dr. Janish Patel and Dr. Kimberly Blasius.
Dr Albert Chan from shares practical tips & resources for using simulation for Covid19 airway management based on the Hong Kong experience.

Who has won the seven year bet on video laryngoscopy versus the old Mac? Let's find out - with a little help from The Terminator.

A 28 year old with reduced GCS after several seizures requires intubation. Their neck extension seems limited and you wonder whether this may be a difficult intubation. You decide to monitor it with ultrasound.

INDICATIONS A – protection and patencyB – respiratory failure (hypercapnic or hypoxic), increase FRC, decrease WOB, secretion management/ pulmonary toilet, to facilitate bronchoscopyC – minimise oxygen consumption and optimize oxygen delivery (e.g. sepsis)D – unresponsive to pain, terminate seizure, prevent…
Post-intubation hypoxia can be rapidly fatal without early intervention, which requires a structured approach to concurrently identifying and treating the underlying cause