
![]()
Thomas Lewis
Sir Thomas Lewis (1881-1945) was a Welsh cardiologist.
Lewis was a pioneering British cardiologist, clinical scientist, and physiologist renowned for establishing clinical cardiac electrophysiology and advancing the science of vascular responses and pain. Born on December 26, 1881, in Cardiff, Wales, Lewis demonstrated an early academic brilliance and attended University College London (UCL), where he trained in medicine and physiology. He graduated MBBS with distinction in 1905 and quickly immersed himself in experimental medicine.
Lewis’s career was profoundly shaped by his collaboration with Ernest Starling (1866–1927) and his mentorship under prominent physiologists such as E.H. Starling and W.H. Bayliss. Early on, he focused on the mechanisms of the heartbeat and became one of the first physicians to use the electrocardiogram (ECG) to study arrhythmias, particularly auricular fibrillation—a term he helped to define and characterise. His 1920 publication, The Mechanism and Graphic Registration of the Heart Beat, laid the foundation for modern electrocardiography and remains a landmark in cardiology.
During World War I, Lewis’s attention turned to the mysterious syndrome afflicting soldiers—marked by fatigue, palpitations, and breathlessness—which was often misattributed to malingering. He identified it as “effort syndrome,” linking it to cardiovascular deconditioning rather than psychological weakness. His work dramatically changed the treatment and understanding of wartime neurosis and fatigue syndromes.
Lewis was the author of numerous articles and textbooks including Clinical Disorders of the Heart Beat (1912 – seven editions), Clinical electrocardiography (1913 – six editions), The soldier’s heart and the effort syndrome (1918), The mechanism and graphic registration of the heart beat (1920). His work received widespread recognition and awards including The Royal Society (Royal Medal, 1927 and Copley Medal, 1941); Royal College of Physicians (Conway Evans Prize); C.B.E. (1920) and knighted in 1921.
In later life he later focused his energies on the study of pain, the cutaneous circulation, and vascular reflexes, publishing extensively on the Lewis Triple Response (1927).
Biography
- Born December 26, 1881 in Cardiff, Wales
- 1902 – BSc with first-class honours in both anatomy and physiology, University College, Cardiff
- 1904 – Graduated MBBS with first-class honours, University College Hospital, London
- 1906 – Appointed House Physician, University College Hospital (UCH); Beit memorial fellowship (1910); lecturer in cardiac pathology (1911)
- 1909 – Co-founder with Sir James Mackenzie of the journal Heart; Chief editor from its inception, and after renamed to Clinical Science (1933) and until 1944
- 1914 – after visiting the United States, made a study of heart affections in warfare for the Medical Research Committee and became consulting physician on heart diseases to Eastern Command
- 1915 – Identified and described “Effort Syndrome” (aka Da Costa Syndrome) in WWI soldiers
- 1918 – Appointed Director of Medical Research Council Clinical and Physiological Department at UCH
- 1920 – Published major studies on cardiac arrhythmias, including atrial fibrillation
- 1921 – Knighted for services to medicine
- 1924 – Published studies on cutaneous circulation and the vascular response to injury
- 1927 – Suffered first heart attack and gave up his ’70 a day’ smoking habit recognising before others did that ‘smoking injures the blood vessels.’
- 1935 – Suffered a second heart attack and remarked ‘..another arrow from the same quiver my friend, and one of them will get me in the end‘
- 1940 – Retired from University College Hospital
- Died on March 17, 1945 of myocardial infarction. Buried in Llangasty churchyard, Breconshire, Wales, overlooking Llangorse Lake, where he fished and studied nature as a young boy.
Einthoven acknowledged Lewis in his 1925 Nobel Prize acceptance speech:
…Thomas Lewis, who has played a great part in the development of electrocardiography deserves a special mention. It is my conviction that the general interest in ECG would certainly not have risen so high, nowadays, if we had had to do without his work, and I doubt whether without his valuable contributions I should have the privilege of standing before you today.
Einthoven 1925
Medical Eponyms
Lewis lead (S5-lead) (1913)
The Lewis lead configuration is a modified limb lead configuration that accentuates atrial activity, originally developed to assess atrial fibrillation. It is used to better detect atrial activity in relation to that of the ventricles.
P waves (atrial activity) are usually are much less apparent than ventricular activity. The Lewis lead can be of value in amplifying these waves in observing flutter waves in atrial flutter; clarifying the mechanism of an atrial arrhythmia; and detecting P waves in wide complex tachyarrhythmia to identify atrioventricular dissociation.
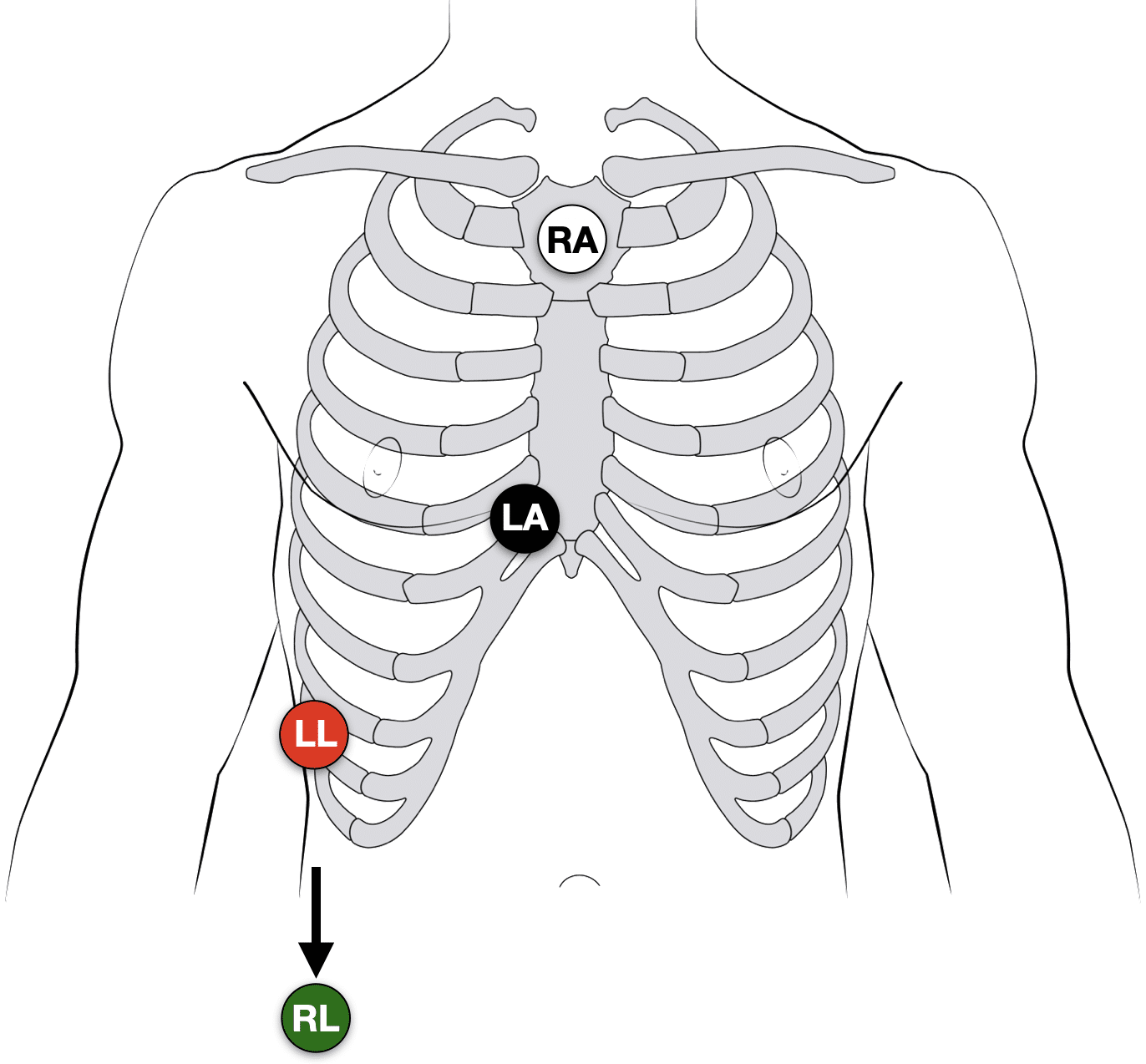
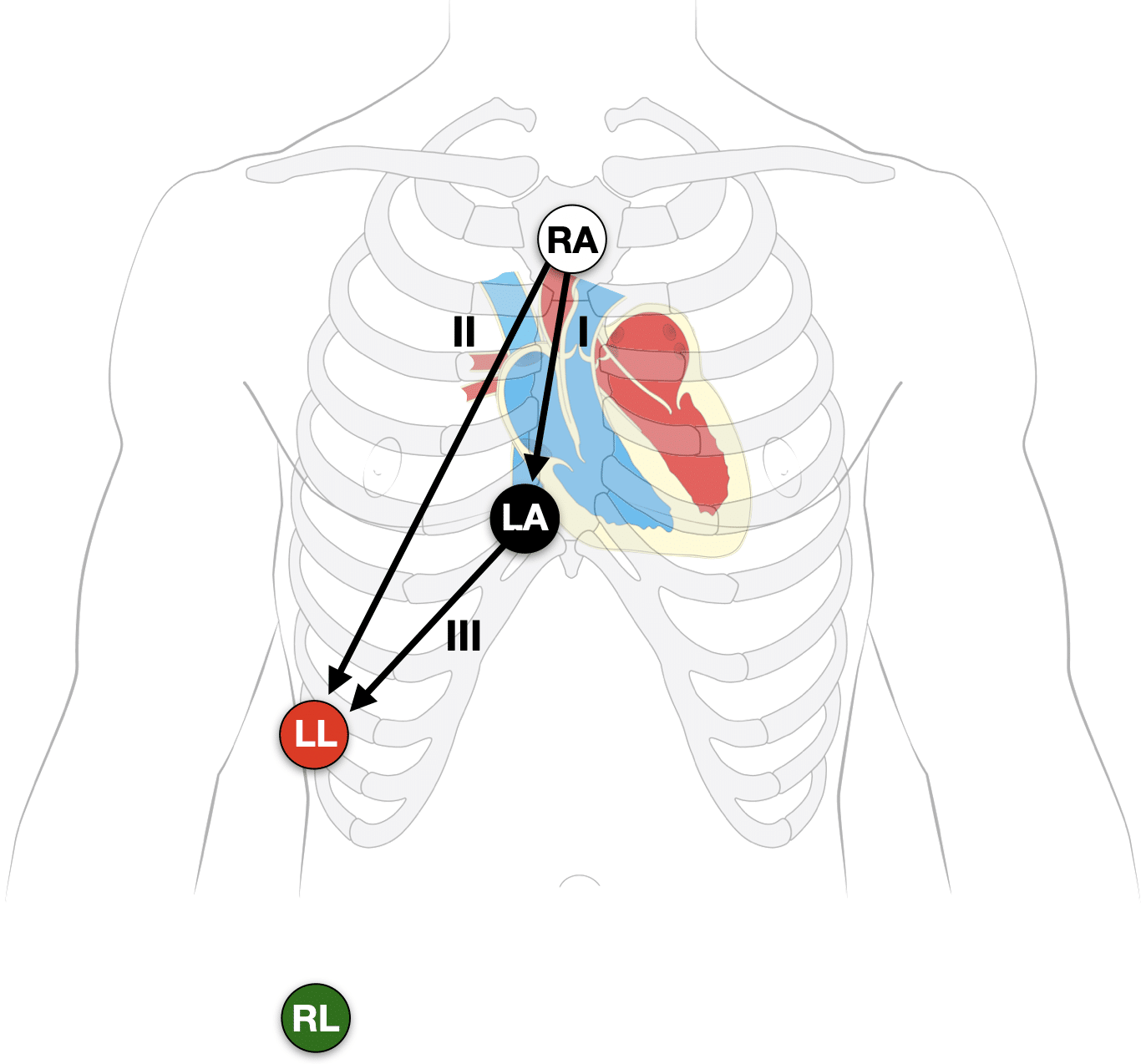
Lewis lead placement
- Right Arm (RA) electrode on manubrium
- Left Arm (LA) electrode over 5th ICS, right sternal border.
- Left Leg (LL) electrode over right lower costal margin.
- Right Leg (RL) electrode in standard position on right leg
- Monitor Lead I and II
Note: Increasing calibration from 10 to 20mm/mV; and paper speed from 25 to 50mm/second can further amplify the atrial activity
History of the Lewis Lead
Thomas Lewis developed and described (1913) his lead configuration to magnify atrial oscillations present during atrial fibrillation.
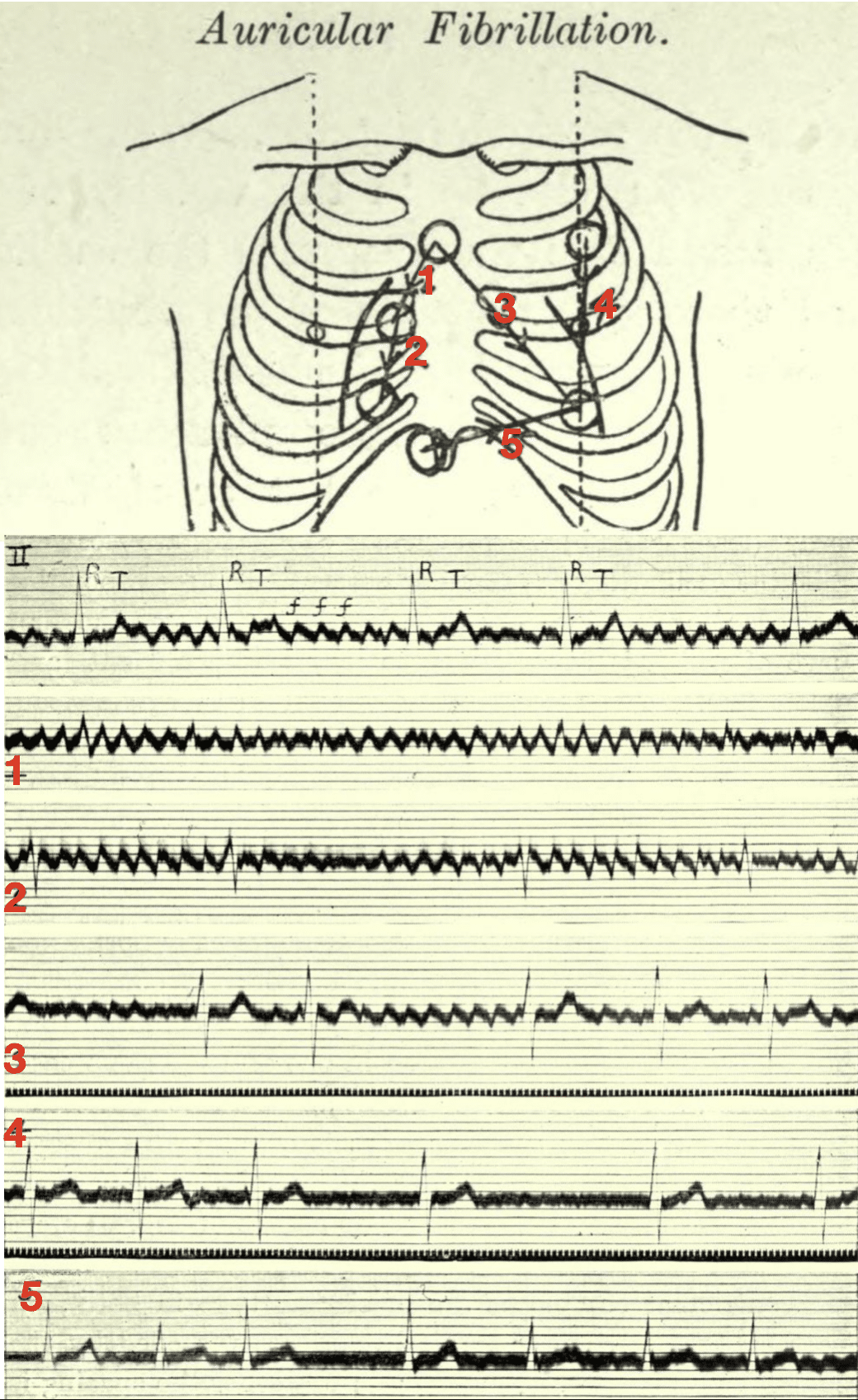
When fibrillation is present and the electrodes lie in the vicinity of the right auricle (leads 1 and 2 of the diagram) the oscillations are maximal, and there is but a trace of the ventricular beats. When they lie in the long axis of the heart (lead 3) then both the oscillations and the ventricular complexes are conspicuous. Finally, when they lie along the left or right ventricular border (leads 4 and 5) the ventricular complexes are clear cut while the oscillations are small or absent.
The corresponding electrocardiograms are shown below the diagram, the first curve of which is from the customary lead II (right arm to left leg). The oscillations of fibrillation are readily identified in this manner and their origin in the auricle is clearly indicated. In tremulous subjects, no oscillations are seen in any of the special leads.
Lewis 1913
Lewis T. Auricular fibrillation 1913
The first electrocardiogram is from lead II; it consists of irregularly placed ventricular complexes (R, T) and of large and continuous oscillations (f f).
The remaining five curves are from the chest wall.
- 1 and 2 were taken from the area overlying the right auricle; in these leads the oscillations are maximal and the ventricular complexes are minimal.
- 3 was taken from an oblique lead covering the whole heart, and it shows both oscillations and ventricular complexes.
- 4 and 5 were taken from leads along the margins of the ventricles; they show but little sign of the oscillations.
Lewis Triple Response (1927)
A classic neurogenic inflammatory skin reaction comprising three sequential phenomena following firm stroking of the skin: a red line, a surrounding flare, and a wheal.
The phenomenon offers insight into normal and pathological cutaneous physiology. It illustrates how vascular reactivity and sensory nerves interact and aids in diagnosing systemic diseases affecting skin innervation or immune-mediated vascular activity.
Phases and Mechanisms
- Red spot (~5–15 s): Local capillary vasodilation from direct mechanical stimulation.
- Flare (~30–45 s): Surrounding arteriolar dilation via axon reflex—antidromic impulses trigger histamine release and neuropeptides like substance P and CGRP
- Wheal (~1–3 min): Plasma leakage and edema from increased permeability of postcapillary venules due to histamine
Clinical insights
- Dermatographism/urticaria: An exaggerated triple response suggests histamine hyper-reactivity.
- Autonomic dysfunction or neuropathy: Absent or diminished response may indicate impaired axon reflex pathways
First described by Lewis in 1924 as a tool to study cutaneous vascular and neurogenic responses and published in 1927
The full reaction to stroking, namely, the local vasodilatation, the flare and eventually local edema, constitutes what I shall henceforth call the triple response
Cutaneous vascular response to trauma formed the basis for understanding neurogenic inflammation and continues to be used in physiological teaching.
Key Medical Contributions
Electrocardiography and Cardiac Arrhythmias
Lewis was one of the first to introduce the clinical electrocardiogram in the UK. His work provided systematic classifications and explanations for cardiac arrhythmias, including atrial fibrillation and heart block. His books Clinical electrocardiography (1913) and The mechanism and graphic registration of the heart beat, remain landmark publications in cardiology
Effort Syndrome (Soldier’s Heart)
During WWI, Lewis studied soldiers suffering from unexplained fatigue, tachycardia, and breathlessness. He showed these symptoms stemmed from cardiovascular deconditioning rather than psychological causes, leading to a paradigm shift in understanding combat fatigue.
Lewis expanded upon the 1871 observations of Jacob Mendez Da Costa (1833-1900) and his “irritable heart or Da Costa syndrome,” a condition mimicking heart disease but distinctly functional. In 1918, Lewis authored The soldier’s heart and the effort syndrome, renaming the condition “effort syndrome” after noting its strong link to physical exertion.
Lewis highlighted a homeostatic failure in acid-base buffering during activity and theorised that reduced buffering capacity led to early fatigue—an idea later supported by studies showing low anaerobic thresholds and hyperventilation-induced acidosis in affected patients.
Effort syndrome remains a useful diagnosis for exercise-induced performance failure due to buffering system dysfunction
Pain and Referred Pain
In later life, Lewis explored the physiology of Pain (1942), including angina and referred pain patterns. He emphasised the role of the sympathetic nervous system in chronic pain states and vascular disorders.
Major Publications
- Lewis T. Auricular fibrillation: A common clinical condition. Br Med J 1909; 2: 1528
- Lewis T. Auricular fibrillation and its relationship to clinical irregularity of the Heart. Heart 1910; 1(4): 306–372.
- Lewis T. The mechanism of the heart beat with especial reference to its clinical pathology. London, Shaw. 1911
- Lewis T. Clinical disorders of the heartbeat. London, Shaw. 1912
- Lewis T. Clinical electrocardiography. London, Shaw. 1913
- Lewis T. Lectures on the heart. New York P.B. Hoeber 1915
- Lewis T. The spread of the excitatory process in the vertebrate heart. Parts I-V. Philosophical Transactions of the Royal Society B 1916; 207
- Lewis T. The soldier’s heart and the effort syndrome. London, Shaw. 1918
- Lewis T. The mechanism and graphic registration of the heart beat. London, Shaw. 1920
- Lewis T. The Blood Vessels of the Human Skin and Their Responses. 1927
- Lewis T. Clinical science: illustrated by personal experiences. London, Shaw. 1934
- Lewis T. Pain. 1942
- Lewis T. Reflections upon reform in medical education. Lancet 1944; 243(6298): 619–621
- Lewis T. Diseases of the heart : described for practitioners and students. 1946
References
Biography
- Sir Thomas Lewis (1881-1945) experimental cardiologist. JAMA. 1966 Mar 21;195(12):1055-6.
- Burchell H. Sir Thomas Lewis: his impact on American cardiology. Br Heart J. 1981 Jul;46(1):1-4.
- Hollman A. Thomas Lewis: physiologist, cardiologist, and clinical scientist. Clin Cardiol. 1985 Oct;8(10):555-9.
- Hollman A. Sir Thomas Lewis: Clinical Scientist and Cardiologist, 1881–1945. Journal of Medical Biography, 1994; 2(2), 63–70.
- Davies MK, Hollman A. Sir Thomas Lewis (1881-1945). Heart. 1996 Nov;76(5):383.
- Krikler DM. Thomas Lewis, a father of modern cardiology. Heart. 1997; 77(2): 102–103.
- Hollmann A. Sir Thomas Lewis: Pioneer Cardiologist and Clinical Scientist. Springer. 1997
- Haas LF. Sir Thomas Lewis 1881-1945. J Neurol Neurosurg Psychiatry. 2005 Aug;76(8):1157.
- Pearce JM. Sir Thomas Lewis MD, FRS. (1881-1945). J Neurol. 2006; 253(9): 1246-7
- Biography: Sir Thomas Lewis. Inspiring Physicians. Royal College of Physicians of London
Eponymous terms
- Kong LN. The triple response of Lewis. Med Bull (Ann Arbor). 1960 Dec;26:445-50.
- Xiao HB, Lawrence C. Reappraisal of Thomas Lewis’s place in the history of electrocardiography. J Electrocardiol. 1996; 29(4): 347-50
- Nahm F, Freeman R. Vasovagal syncope: the contributions of Sir William R. Gowers and Sir Thomas Lewis. Arch Neurol. 2001; 58(3): 509-511.
- Bakker AL, Nijkerk G, Groenemeijer BE, Waalewijn RA, Koomen EM, Braam RL, Wellens HJ. The Lewis lead: making recognition of P waves easy during wide QRS complex tachycardia. Circulation. 2009 Jun 23; 119(24): e592-3
- Buttner R, Cadogan M. Lewis Lead. LITFL
- Cadogan M. History of the Electrocardiogram. LITFL
Eponym
the person behind the name
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |