![]()
Who’s Afraid Of The Big Bad Wolff?
A 61 year old male walks up to the triage desk complaining of a funny feeling in his chest. He has had similar milder episodes in the past and has been investigated by his GP with no firm diagnosis being reached.
He’s moved to Resus as he’s a bit pale and sweaty. His ECG is shown below:
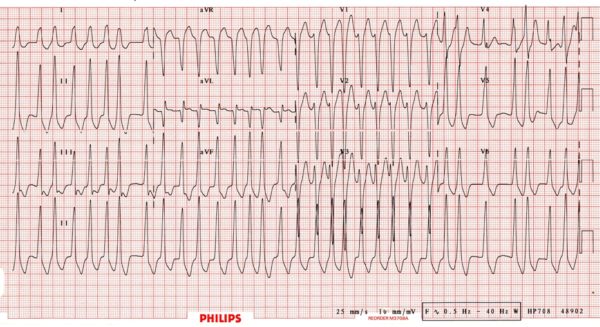
Initially you wonder if it might be Ventricular tachycardia (VT) as it seems broad and fast and initially seems regular, however after watching the monitor for a bit and stroking your Mo, you become convinced the rhythm is actually irregular.
You decide he’s on the ‘unstable’ side of the spectrum and perform DC Cardioversion. Post Cardioversion, his ECG looks like this:
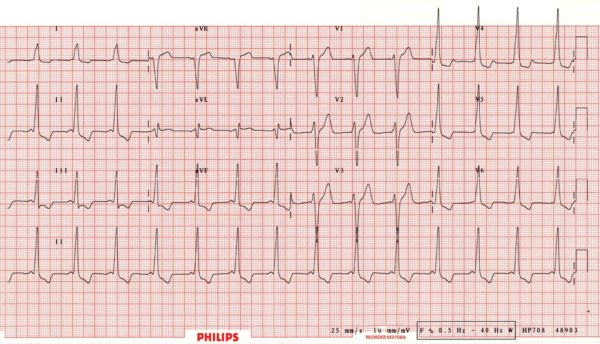
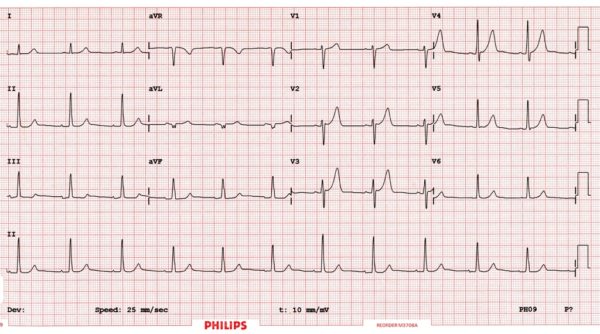
He’s admitted under the care of Cardiology who perform an ablation. Post ablation his ECG looks like this:
Wolff-Parkinson-White Syndrome
ECG pattern depends on where the accessory pathway inserts.
Classically:
- Short PR interval <120 msecs.
- QRS > 100msecs.
- Delta wave = slurred upstroke at beginning of QRS.
Different insertions:
- Normal QRS if pathway inserts into infranodal conduction tissue just below AV node
- Grossly wide and abnormal QRS if pathway inserts into non-conduction tissue.
Key Management Points:
- A heart rate ≥ 200 should make you think of a pre-excitation syndrome.
- Narrow complex SVT is treated identically to non-WPW SVT.
- Don’t try and be clever with drugs in broad complex tachycardias and WPW.
- Using AV nodal blockers in WPW and AF can result in 1:1 conduction to the ventricles.
- This is also know as Ventricular Fibrillation.
- Just shut-up + DC cardiovert them.
References
- Pre-Excitation Syndromes
- VT vs SVT with aberrancy
- The Delta Wave: ECG Basics
- Puzzling Paroxysmal Palpitations
BA MA (Oxon) MBChB (Edin) FACEM FFSEM. Emergency physician, Sir Charles Gairdner Hospital. Passion for rugby; medical history; medical education; and asynchronous learning #FOAMed evangelist. Co-founder and CTO of Life in the Fast lane | On Call: Principles and Protocol 4e| Eponyms | Books |