
![]()
Seventh Cranial Nerve Lesions
Cranial nerve VII is also known as the Facial nerve.
Lesions of the Facial nerve are relatively common compared to other cranial nerve lesions.
Lesions of the Facial nerve may present as:
- Lower motor neuron (LMN) lesions — due to both central and peripheral causes
- Upper motor neuron (UMN) lesions — typically part of a central stroke syndrome
Commonest causes:
- UMN: Cortical stroke
- LMN: Bell’s palsy
Anatomy
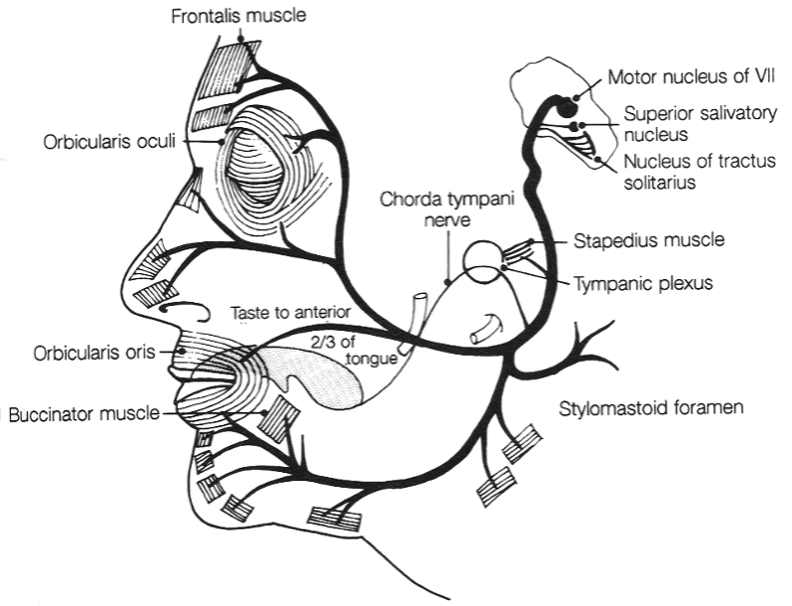
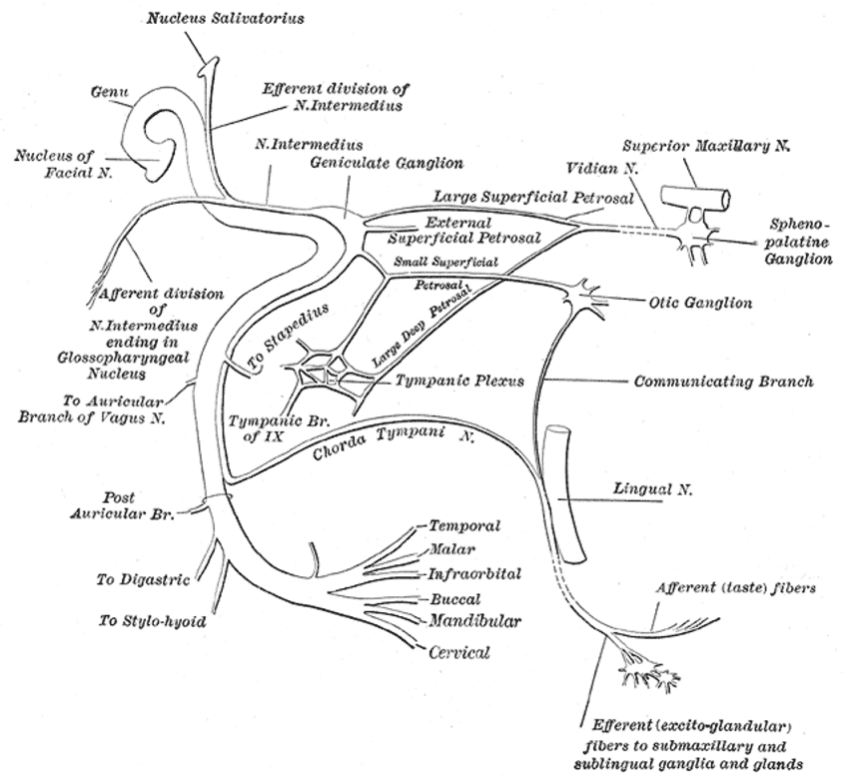
Course of the Facial Nerve
- Somatic efferent fibres originate in the facial nucleus (pons)
- Upper face muscles: bilateral cortical innervation
- Lower face muscles: contralateral cortical innervation
→ In UMN lesions → forehead spared; in LMN lesions → complete ipsilateral facial paralysis
- Emerges from ventral brainstem (junction of pons and medulla)
- CN VI emerges medial
- CN VIII emerges lateral
- Travels in posterior cranial fossa, enters facial canal via internal acoustic meatus with CN VIII + labyrinthine artery
- Facial canal → geniculate ganglion → joined by chorda tympani
- Exits via stylomastoid foramen → passes through parotid gland → divides into terminal branches
Facial Nerve Innervations
| Branch location | Branches | Innervation |
|---|---|---|
| Facial canal | Greater petrosal nerve | Lacrimal gland, nasal glands, palatal glands |
| Nerve to stapedius | Stapedius muscle | |
| Chorda tympani | Taste (anterior 2/3 tongue), submandibular & sublingual glands | |
| Post-canal, pre-parotid | Nerve to posterior belly of digastric | Digastric muscle |
| Branches to auricular muscles, occipitofrontalis | Scalp and ear muscles | |
| Nerve to stylohyoid muscle | Stylohyoid muscle | |
| Within parotid gland (Mnemonic: Two Zebras Bit My Cake!) | Temporal | Muscles of forehead/scalp |
| Zygomatic | Muscles around eye | |
| Buccal | Upper lip, nose, buccinator | |
| Mandibular | Lower lip, chin | |
| Cervical | Platysma |
Pathology
Upper Motor Neuron (UMN)
| Cause |
|---|
| Cortical strokes (middle cerebral artery territory) |
Lower Motor Neuron (LMN)
| Site | Cause |
|---|---|
| Brainstem (pons) | Stroke, demyelination (MS), tumour |
| Cerebello-pontine angle | Acoustic neuroma, meningioma, meningitis |
| Middle ear | Infections, tumours (affects chorda tympani) |
| Trauma | Petrous temporal bone fracture, penetrating nerve trauma |
| Infections | Bell’s palsy, Ramsay-Hunt syndrome (HZV), tetanus, tick paralysis |
| Parotid gland | Tumour, abscess, trauma/surgery |
| Rare mononeuritis | Connective tissue disease, diabetes, alcohol, paraneoplastic, sarcoidosis, HIV |
Clinical Assessment
1. Inspect for Facial Asymmetry
Look for:
- Unilateral drooping of mouth
- Unilateral smoothing of forehead wrinkles
- Unilateral loss of nasolabial fold
2. Test Forehead (Frontalis) Muscles
- Ask patient to look upwards → observe forehead wrinkles
- Apply downward pressure to test strength
| Finding | Indicates |
|---|---|
| Forehead movement spared | UMN lesion |
| Forehead + lower face paralysis | LMN lesion |
3. Test Orbicularis Oculi (Eye Muscles)
- Ask patient to close eyes tightly
- Attempt to force open eyes
| Finding | Indicates |
|---|---|
| Eye closure weak + Bell’s phenomenon | LMN lesion |
4. Show Teeth
- Ask patient to show teeth
- Compare nasolabial folds
| Finding | Indicates |
|---|---|
| Nasolabial fold loss on same side | LMN lesion |
| Nasolabial fold loss on opposite side | UMN lesion |
5. Check for Vesicular Lesions
- Inspect external ear, auditory canal, palate
- Presence suggests Ramsay-Hunt syndrome
6. Taste Testing (if required)
- Apply one taste stimulus to each side of anterior 2/3 tongue:
| Taste | Substance |
|---|---|
| Sweet | Sugar |
| Sour | Vinegar |
| Bitter | Quinine |
| Salty | Saline |
Rinse mouth between tests.

Note the complete loss of the nasolabial groove on the (patient’s)left. Failure to close the eye on the left would confirm a lower motor lesion of the left facial nerve, (photo from the Photo Science Library Website, http://www.sciencephoto.com/).
Nerve Conduction Studies
- Can be done for Facial nerve
- Some prognostic value in Bell’s palsy
- Not routinely performed
Investigations
Blood Tests
- FBC
- U&Es / glucose
- CRP
- ESR
- Additional tests as indicated (e.g. blood lead levels)
CT Scan / CT Angiogram
- Screening for intracranial mass lesions
- CT angiogram → suspected aneurysm
MRI
- Best for:
- Mass lesions
- MS plaques
- Middle ear pathology
- Visualisation of the facial nerve
Management
- Directed at the underlying cause
Eye Care
- Major complication of LMN lesion → incomplete eye closure → corneal ulceration risk
- Management:
- Artificial tear drops
- Protective eye pads
- Lateral tarsorrhaphy (in severe cases)
Psychological Support
- May be needed due to the disfiguring nature of the lesion
Appendix 1
Appendix 2
References
Publications
- Brazis PW, Masdeu JC, Biller J. Localization in Clinical Neurology. 8e 2021
- Fuller G. Neurological Examination Made Easy. 6e 2019
- O’Brien M. Aids to the Examination of the Peripheral Nervous System. 6e 2023
FOAMed
- Sanger G. Bell’s Palsy. LITFL
- Cadogan M. Ramsay Hunt syndrome. LITFL
- Coni R. Neuro 101: Cranial Nerves. LITFL
- Nickson C. The Brainstem Rules of Four. LITFL
- Ercleve T. The rule of 4 of the brainstem. LITFL
- Nickson C. Cranial nerve lesions DDx. LITFL
Fellowship Notes

MBBS DDU (Emergency) CCPU. Adult/Paediatric Emergency Medicine Advanced Trainee in Melbourne, Australia. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Co-creator of the LITFL ECG Library. Twitter: @rob_buttner

Educator, magister, munus exemplar, dicata in agro subitis medicina et discrimine cura | FFS |