
![]()
Anatomy for bronchoscopy
Anatomy for bronchoscopy and airway management
Overview
Airway anatomy is highly relevant to diagnosis and management in critical care.
- this includes both the upper airway (e.g. laryngoscopy, threats to airway patency and protection) and the lower airway (e.g. bronchoscopy and respiratory pathology)
- bronchoscopic anatomy follows the airway from the vocal cords to the segmental bronchi.
The bronchoscopist navigates from within the airway using a series of landmarks to maintain orientation, localise pathology and safely perform procedures.
- You don’t need to know anatomy, you need to be able to find it!
- Safe bronchoscopy depends on three skills:
- maintaining orientation
- recognising normal anatomy and common variants
- identifying abnormalities
Many apparent abnormalities are simply normal variants. Equally, important disease is often identified because the airway has an abnormal appearance.
Bronchoscopy Roadmap
Most bronchoscopic examinations follow the same sequence:
- Upper airway (unless intubated)
- Vocal cords (unless intubated)
- Trachea
- Carina
- Right main bronchus
- Right upper lobe
- Bronchus intermedius
- Right middle lobe
- Right lower lobe
- Left main bronchus
- Left upper lobe
- Lingula
- Left lower lobe
If orientation is lost, return to the carina and restart from there.
Bronchoscopic Orientation
Know how to maintain orientation is vital – if in doubt always come back to the carina:
- The carina is your compass
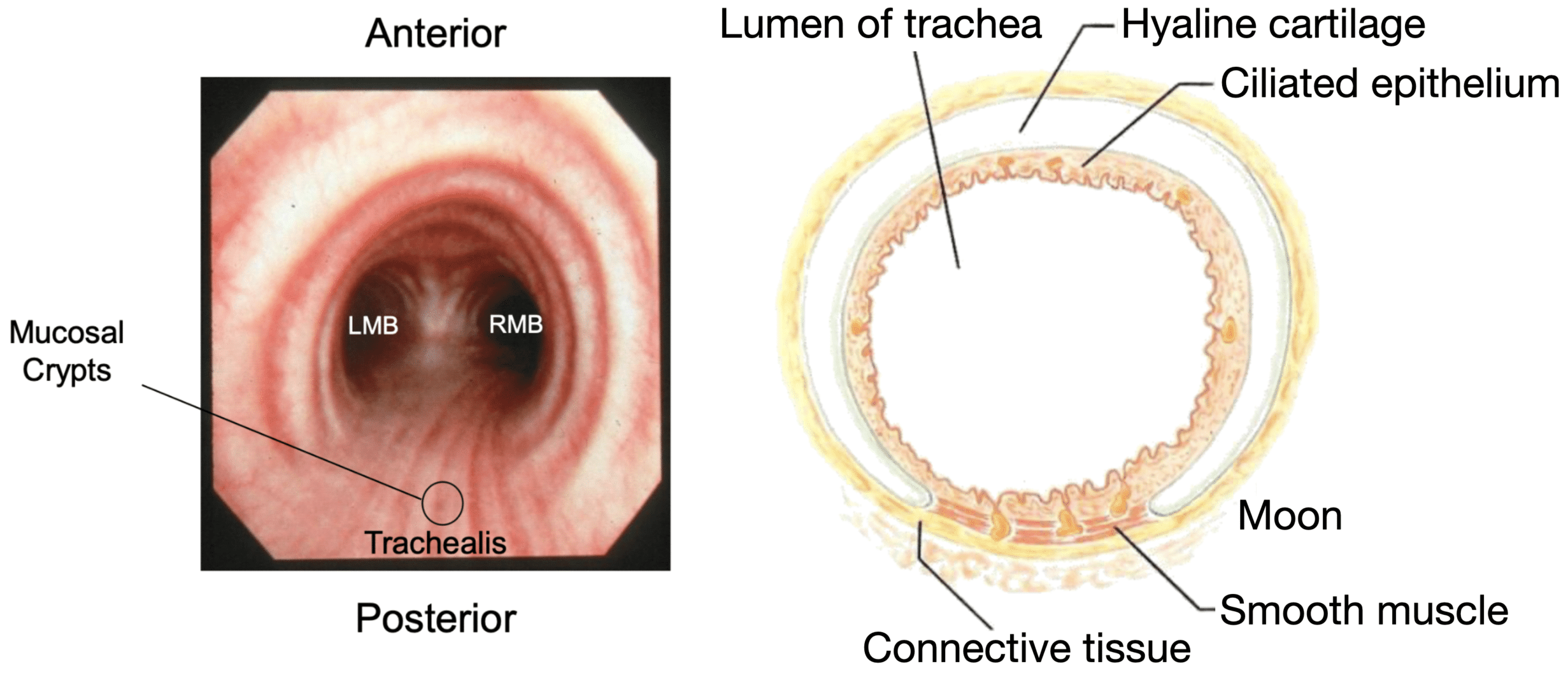
- The trachea is D-shaped, cartilage is anterior, and membrane is posterior
Use the following landmarks continuously:
- posterior membrane (has characteristic “racing stripes” from the longitudinal striations of the trachealis muscle)
- main carina
- secondary carinae
- major airway branches
Remember:
- upper lobes branch superiorly
- lower lobes branch inferiorly
- the right bronchial tree is more vertical (almost continuous with the trachea)
- the left bronchial tree is more horizontal
Upper Airway
The upper airway and larynx are functionally important for:
- Respiration
- Humidification
- airway protection
- Phonation, and
- procedural access in critical care
A useful navigation sequence is:
- Uvula → Epiglottis → Larynx
- particularly useful when secretions, blood or distorted anatomy obscure normal landmarks.
The laryngeal inlet is the opening from the pharynx into the larynx. It is bounded by:
- Epiglottis (anterior)
- Arytenoids + interarytenoid notch (posterior)
- Aryepiglottic folds (lateral)
Vallecula, hyoepiglottic ligament, and glottic exposure
- The epiglottis is the “gateway to the larynx” during laryngoscopy
- The epiglottis is connected to the hyoid by the hyoepiglottic ligament
- Seating the tip of the laryngoscope blade in the vallecula (anterior to the epiglottis) activates (stretches) the hyoepiglottic ligament and causes the epiglottis to lift anteriorly exposing the glottis
- Failure to do this correctly is a common reason for poor laryngoscopic view
The vocal cords sit below the laryngeal inlet. They form the glottis and divide the upper airway from the lower airway. Unless paralysed, they provide a dynamic sphincter that the bronchoscopy must negotiate.
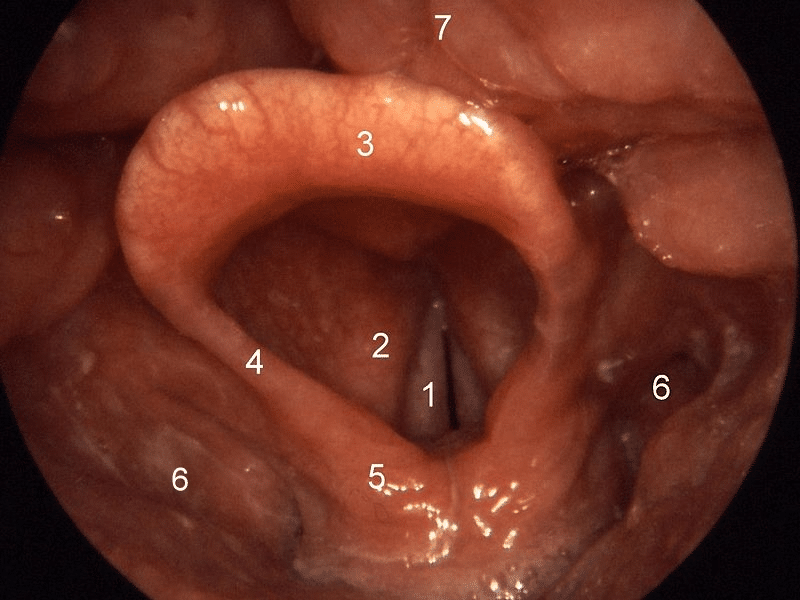
Structures labelled: 1 = vocal chords, 2 = vestibular fold (“false cords”), 3 = epiglottis, 4 = aryepiglottic folds, 5 = arytenoid cartilage, 6 = sinus piriformis, 7 = base of the tongue.
Image by Welleschik available at: https://commons.wikimedia.org/wiki/File:Larynx_normal.jpg
{kind=link}
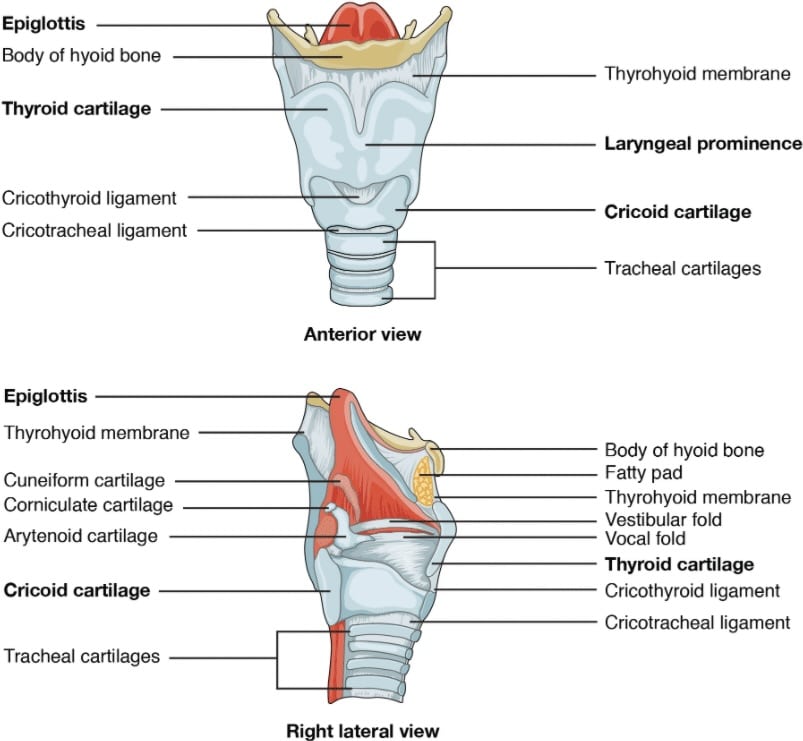
Image from Fundamentals of Anatomy and Physiology by Anna Chruścik; Kate Kauter; Louisa Windus; and Eliza Whiteside available at: https://usq.pressbooks.pub/anatomy/chapter/8-1-organs-and-structures-of-the-respiratory-system/
The cricoid cartilage forms the boundary between larynx and trachea.
- lies immediately below the vocal cords and above the first tracheal ring
- It is the only complete cartilaginous ring in the airway
- It is shaped like a signet ring resulting in a broad cartilagenous wall posteriorly
- This makes it an important landmark during:
- Front of neck access (cricothyroidotomy and tracheostomy)
- airway stenosis assessment
- interventional airway procedures
- The cricothyroid membrane lies anteriorly, between the cricoid cartilage and the thyroid cartilage
Common upper airway normal variants include:
- omega-shaped epiglottis (may be more common in obesity)
- prominent arytenoids
- variation in glottic size
Upper airway landmarks are not visible when bronchoscopy is performed in a patient who is already intubated. Only the features of the endotracheal tube (ETT) will be visible as the bronchoscope pass along it:
- Clear plastic cylindrical tube lumen
- external depth markings on ETT may be visible
- Murphy’s eye near distal tip of ETT
Trachea
The trachea extends from the cricoid cartilage to the carina.
- Healthy trachea shows C‑shaped anterior cartilaginous rings with a membranous posterior wall.
- The adult trachea contains approximately 16-20 cartilaginous rings.
- Usually 10-12 cm in length in adults (from C6 to T4/5 level)
For bronchoscopy, only a few features truly matter:
- cartilage anteriorly
- membrane posteriorly
- slight rightward deviation approaching the carina
- dynamic movement during breathing and coughing
Important adjacent structures (especially relevant for FONA procedures)
- Anterior
- Great vessels
- Brachiocephalic (innominate) artery – crosses anterior to the upper thoracic trachea
- Brachiocephalic (innominate) vein – passes anterior to the trachea in the superior mediastinum
- Distally
- Aortic arch – lies anterior and to the left of the distal trachea
- Superior vena cava (SVC) – lies anterolateral to the right side of the trachea
- Pulmonary trunk – lies anterior to the distal trachea and carina
- Thyroid and vessels
- Thyroid isthmus crosses the anterior surface of the trachea at the level of the 2nd–4th tracheal rings
- The inferior thyroid veins descend anterior to the upper trachea and drain into the brachiocephalic veins.
- The thyroid ima artery (when present; anatomical variant) ascends on the anterior trachea, usually arising from the brachiocephalic trunk or aortic arch.
- Great vessels
- Lateral
- Recurrent laryngeal nerves run bilaterally along the trachea
- Branches of the inferior thyroid arteries run posterolateral to the trachea near the recurrent laryngeal nerves.
- The thyroid lobes lie on either side of the upper trachea and extend posteriorly towards the oesophagus and carotid sheath
- Posterior
- Esophagus
These adjacent structures can distort the airway through:
- Masses (e.g. goitre, tumours)
- lymphadenopathy
- fibrosis
- previous surgery
- Vessel enlargement (e.g. aneurysm, SVC obstruction)
Mild dynamic movement of the posterior membrane during expiration is normal
- Trachealis muscle contracts and constricts trachea during coughing
- Excessive expiratory collapse of the airway is abnormal and may indicate:
- Tracheobronchomalacia – weakness of the cartilaginous airway wall.
- Excessive Dynamic Airway Collapse (EDAC) – exaggerated inward bulging of the posterior membranous wall.
A tracheal bronchus (“pig bronchus”) is an anatomical variant that arises directly from the trachea above the carina and usually supplies part of the right upper lobe.
- Occurs in 0.1-2% of people, usually discovered incidentally
- Recognition is important because it may affect:
- endotracheal tube positioning
- lung isolation and one-lung ventilation
- bronchoscopic navigation and interpretation
Carina
The carina is the most important landmark in bronchoscopy.
- It is the bifurcation between the right and left main bronchi
- Experienced bronchoscopists continually return to the carina to maintain orientation.
At the carina:
- the right main bronchus is shorter, wider and more vertical
- the left main bronchus is longer, narrower and more horizontal
- the posterior membranous wall identifies posterior orientation
- the cartilaginous wall identifies anterior orientation
The carina lies within the middle mediastinum and is surrounded by structures commonly encountered during bronchoscopy, EBUS and transbronchial needle aspiration. Important relationships include:
- Anterior: pulmonary trunk and origin of the right and left pulmonary arteries
- Posterior: oesophagus and descending thoracic aorta
- Inferior: left atrium (which is below subcarinal space (station 7), one of the most frequently sampled lymph node stations during bronchoscopy)
- Right: azygos vein arch and right paratracheal lymph node stations
- Left: aortic arch, aortopulmonary window, and left paratracheal lymph node stations
Unexpected carinal appearances are “red flags” for underlying pathology:
| Finding | Possible Cause |
|---|---|
| Widened carinal angle | Subcarinal lymphadenopathy or other disease outside the airway rather than within it |
| Blunted carina | Malignancy |
| Distorted anatomy | Mediastinal mass |
| Fixed carina | Infiltrative disease |
| Shifted carina | Volume loss or mediastinal displacement |
Mediastinal and Hilar Relations
Lymph Node Stations
- These are less relevant in the ED and ICU setting, but are important in diagnostic bronchoscopy as EBUS and TBNA targets.
- The most important targets are:
| Station | Location |
|---|---|
| 4R | Right lower paratracheal |
| 4L | Left lower paratracheal |
| 7 | Subcarinal |
| 10R | Right hilar |
| 10L | Left hilar |
| 11R | Right interlobar |
| 11L | Left interlobar |
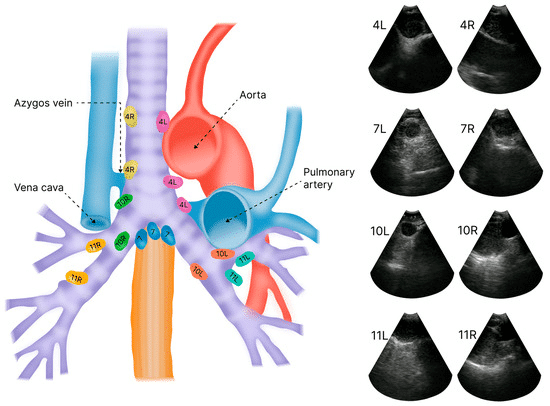
Image source: https://www.mdpi.com/2313-433X/11/1/10
Vascular relations – many are adjacent to lymph node stations – they are important structures to miss when performing biopsies! These relationships are useful for understanding hilar pathology, EBUS anatomy, and mediastinal staging.
- Azygos Vein
- The azygos vein arches over the right main bronchus before entering the superior vena cava.
- It creates an important landmark for:
- station 4R
- right paratracheal anatomy
- upper mediastinal orientation
- Aortopulmonary Window
- Located between aortic arch and left pulmonary artery
- It contains stations 5 and 6 and is an important radiological landmark when correlating CT findings with airway anatomy.
- Pulmonary arteries
- The left pulmonary artery passes superior to the left main bronchus.
- The right pulmonary artery lies anterior to the right main bronchus.
Bronchoscopic Nomenclature
Segmental bronchi are designated using the letter B followed by a number (Boyden classification).
| Segment | Right Lung | Left Lung |
|---|---|---|
| B1 | Apical (RUL) | Apical (LUL upper division) |
| B2 | Posterior (RUL) | Posterior (LUL upper division) |
| B3 | Anterior (RUL) | Anterior (LUL upper division) |
| B4 | Lateral (RML) | Superior lingular |
| B5 | Medial (RML) | Inferior lingular |
| B6 | Superior segment (RLL) | Superior segment (LLL) |
| B7 | Medial basal | Medial basal (often absent on the left) |
| B8 | Anterior basal | Anterior basal |
| B9 | Lateral basal | Lateral basal |
| B10 | Posterior basal | Posterior basal |
Important differences to note in the left lung:
- Left medial basal (B7) is usually absent
- Left apical and posterior (B1 and B2) are often fused (B12 or apicoposterior) or arise from common bronchial trunk.
- lingula segments are rotated in orientation compared to the RML: superior & inferior, instead of lateral & medial
Right Bronchial Tree
The right bronchial tree is shorter, wider, and more vertical than the left. These characteristics contribute to the ease of:
- right mainstem intubation
- right-sided aspiration
- preferential entry of bronchoscopes into the right lung
Right Main Bronchus
- Approximately 2 cm long.
- Rapidly divides into:
- RUL bronchus
- Bronchus intermedius (BI)
Right upper lobe bronchus
- Usually trifurcates into:
- B1 apical
- B2 posterior
- B3 anterior
- This is the first major branch seen on entering the right lung with a bronchoscopy (unless there is a tracheal (“pig”) bronchus.
Bronchus intermedius (BI)
- extends from the RUL take-off to the middle lobe bronchus.
- This is an important orientation pointsin bronchoscopy.
- The anterior wall becomes the middle lobe
- The posterior wall becomes the lower lobe
- Important relationships:
- RML originates anteriorly
- RLL continues posteriorly
- B6 (superior segment) arises posteriorly
Right Middle Lobe
- Typically divides into:
- B4 lateral
- B5 medial
Right Lower Lobe
- The superior segment (B6) arises posteriorly.
- It is a useful landmarks for re-establishing lower-lobe orientation
- The basal trunk typically divides into:
- B7 medial basal
- B8 anterior basal
- B9 lateral basal
- B10 posterior basal
Secondary carinae
- RC1 = RUL–BI carina
- RC2 = RML–RLL carina
Left Bronchial Tree
The left bronchial tree, compared to the right, is longer, narrower, and more horizontal
- Rotate the scope approximately 90° left so the anterior wall lies at around the 3 o’clock position to enter the left upper lobe.
Left Upper Lobe
- Upper Division
- B1 apical
- B2 posterior
- However, while textbooks depict separate B1 (apical), B2 (posterior) and B3 (anterior) segments, fusion of B1 and B2 into a common apicoposterior trunk is common
- B3 anterior
- Lingula
- The lingula is the left-sided equivalent of the middle lobe.
- It divides into:
- B4 superior lingular
- B5 inferior lingular
Left Lower Lobe
- Divides into:
- B6 superior segment
- basal trunk
- The basal trunk typically gives rise to:
- B8 anterior basal
- B9 lateral basal
- B10 posterior basal
- B7 (medial) is usually absent
Secondary carinae:
- LC1 = LUL-LLL
- LC2 = upper division–lingula
Practical tips and pitfalls
Common ICU Bronchoscopy Targets
- Most ICU bronchoscopies involve localisation of secretions, aspiration, bleeding, or airway pathology.
- Knowing the common sites helps direct the examination efficiently.
| Clinical Scenario | Common Anatomical Sites | Bronchoscopic Objective |
|---|---|---|
| Aspiration | Right lower lobe (RLL) Bronchus intermedius Dependent lung segments | Identify and clear aspirated material; assess extent of airway involvement |
| Mucus | Bronchus intermedius Right middle lobe (RML) Lower lobes | Localise and remove obstructing secretions; assess for distal collapse |
| Haemoptysis | Variable; may arise from any lung, lobe or segment | Localise bleeding to the affected lung, lobe and segment before further intervention |
| Difficult Airway Assessment | Vocal cords Subglottic region Trachea Main bronchi | Assess airway anatomy, obstruction, stenosis, injury or distortion |
Different aspects of anatomy are relevant to different procedures:
| Procedure | Key Anatomy |
|---|---|
| Intubation | Epiglottis, cords, cricoid |
| Tracheostomy | Cricoid and tracheal rings |
| Foreign body retrieval | Right main bronchus, bronchus intermedius |
| EBUS-TBNA | Carina, stations 4R, 4L, 7, 10 and 11 |
| Transbronchial biopsy | Segmental bronchi |
| Endobronchial biopsy | Carinae and visible lesions |
| Bronchial blocker placement | Main bronchi and lobar take-offs |
Anatomical variation of the airway and respiratory tract is common. Examples include:
- omega-shaped epiglottis
- prominent arytenoids
- tracheal bronchus
- quadrifurcate RUL branching
- variant lingular branching
- absent left B7
- accessory lower-lobe segments
How to avoid getting lost during bronchoscopy:
- Stop! Do not keep advancing
- Return to the main carina if necessary
- Re-establish orientation – trachea is D-shaped, cartilage is anterior, trachealis/ membrane is posterior
- Proceed deliberately identifying landmarks as you advance
Remember the key principles of bronchoscopy orientation.
- The main carina is your compass
- Trachea is D-shaped, cartilage is anterior, trachealis/ membrane is posterior.
- Upper lobes branch superiorly
- Lower lobes branch inferiorly
- Right main bronchus is short, wide and vertical
- Left main bronchus is long, narrow and horizontal
- The anterior bronchus intermedius wall becomes the RML; the posterior wall becomes the RLL.
- Lingula is conceptually the left middle lobe.
- the superior (B6 or apical) segmental bronchi of the lower lobes are posterior
- Normal variation is common.
- If lost, return to the carina and start again.
Useful videos
Rich Levitan’s lecture on anatomy for emergency management of the airway:
The Bronchoscopy Academy has produced a number of useful videos for understanding airway and bronchoscopic anatomy.
Upper airway and larynx:
Abnormal upper airway:
Trachea:
Trachea abnormalities:
Bronchi:
Anatomy variants:
Conclusion
Finding relevant anatomy and maintaining orientation is critical to successful bronchoscopy and other airway management procedures
- Different aspects of anatomy are relevant to different airway and bronchoscopy procedures
- Anatomical variation is common, however :red flags: for pathology must be identified
- A deliberate approach to airway procedures and bronchoscopy, with identification of landmarks as you go, leads to success
References and Links
LITFL
- CCC – Flexible Bronchoscope
- CCC – Bronchoscopic anatomy
- CCC – Bronchoscopic Foreign Body Removal
- CCC – Bronchoscopy for Percutaneous Tracheostomy
- CCC – Bronchial blockers
- CCC – Bronchoalveolar lavage (BAL)
- CCC – Double lumen endotracheal tube (DLT)
- CCC – Flexible Nasopharyngolaryngoscopy
Journal articles
- Coleman L, et al. Functional anatomy of the airway. Ch 1 in: Hagberg, C. A. (2017). Hagberg and Benumof’s Airway Management E-Book. Netherlands: Elsevier. [google books]
- Ervik Ø, et al. A New Deep Learning-Based Method for Automated Identification of Thoracic Lymph Node Stations in Endobronchial Ultrasound (EBUS): A Proof-of-Concept Study. J Imaging. 2025 Jan 5;11(1):10. doi: 10.3390/jimaging11010010. PMID: 39852323; PMCID: PMC11766424.
- Kavuru MS, et al. Applied Anatomy of the Airways. Ch 4 in Flexible Bronchoscopy, Third Edition, Editors: Wang KP, Mehta AC, Turner Jr JF, Wiley, 2012. [google books]
- Shah P. Atlas of Flexible Bronchoscopy, CRC Press, 2011 [google books]
FOAM and web resources
- Thoracicanaesthesia.com – Virtual bronchoscopy simulator

Critical Care
Compendium
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC
Great! 7218