![]()
Corrosive ingestions
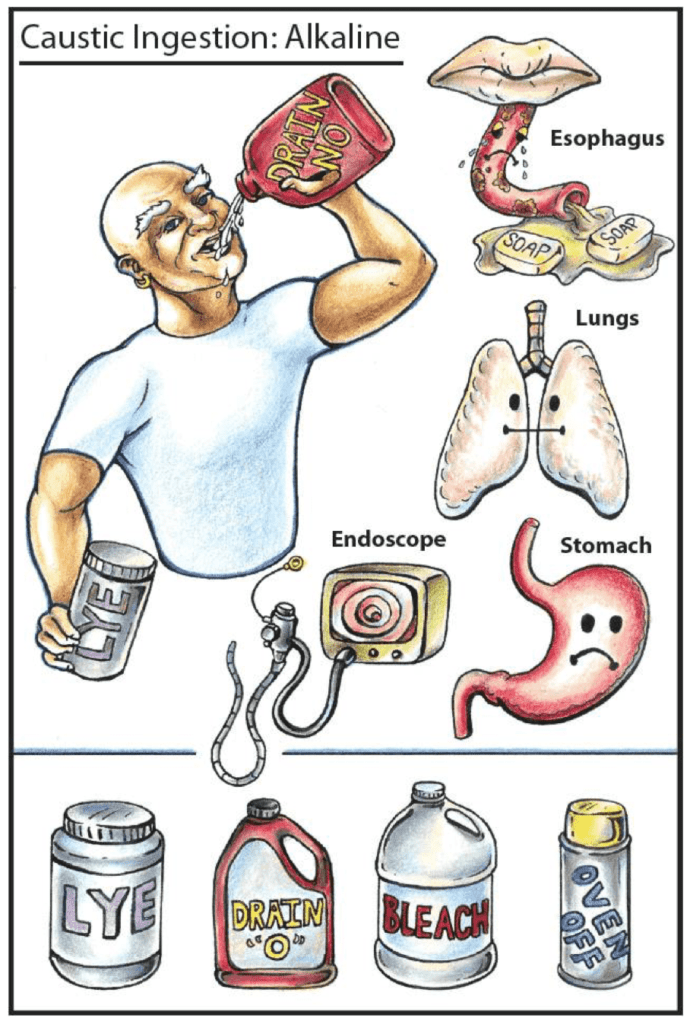
- The common alkalis: Ammonia, Potassium hydroxide, sodium hydroxide, sodium hypochlorite.
- The common acids: Hydrochloric acid, sulphuric acid
- Other agents: Glyphosate, Paraquat, Phenols, Potassium permanganate, mercury chloride, zinc chloride
Toxic Mechanism:
Alkaline agents cause liquefactive necrosis whereas the acids cause protein denaturation and coagulative necrosis.
Resuscitation:
- Potential early life threats include rapid onset of upper airway oedema and compromise requiring early intubation and ventilation.
- Do not insert a nasogastric tube until post endoscopy.
Risk Assessment
- Airway injury is anticipated by the presence of stridor, dysphonia, throat pain, horseless or respiratory distress.
- Gastro-oesophageal injury is indicated by stridor, drooling, vomiting, odynophagia and abdominal pain. If a perforation has occurred then peritonitis will be clinically present with signs of sepsis or multi-system failure.
- Oesophageal perforation or mediastinitis: chest pain, dyspnoea, fever, subcutaneous emphysema and a pleural rub.
- Absence of oral burns does not exclude an ingestion.
- Sulfuric acid or sodium hydroxide either solutions or solid separations cause severe corrosive injury to the pharynx, upper airway, oesophagus and stomach.
- Hydrochloric acid – if concentrated then >60ml leads to severe injury to the stomach and duodenum with necrosis and perforation. Rapid onset of multi-system organ failure and is usually fatal.
- Household bleach – dilute sodium hypochlorite if <150 ml does not cause significant corrosive injury
- Systemic toxicity occurs with: glyphosate, mercuric chloride, paraquat, potassium permanganate and zinc.
- Children: Unintentional ingestion of household bleach is usually benign. Button batteries cause severe corrosive injury if lodged in the oesophagus. Household drain and oven cleaners or automatic dishwashing powders can cause severe corrosive injury.
Supportive Care
- Analgesia
- The symptomatic patient needs to remain nil by mouth until the extent of the injury can be evaluated.
- If there is full thickness necrosis or perforation then broad-spectrum antibiotics and surgical intervention is required.
- If intubated consider FASTHUGSINBED Please (except the NG tube)
Investigations
- Screening: 12 lead ECG, BSL, Paracetamol level
- Specific:
- All patients with persistent vomiting, oral burns, drooling or abdominal pain require further investigation to define the extent of the injury and risk for future complications. This was traditionally an endoscopy within 24 hours but there has been gaining evidence that CT can be used as an alternative within 24 hours.
- Endoscopy grading:
- 0 = Normal
- I = Mucosal oedema and hyperaemia
- IIA = Superfiical ulcers, bleeding and exudates
- IIB = Deep focal or circumferential ulcers
- IIIA = Focal necrosis
- IIIB = Extensive necrosis
- CT grading:
- o = Normal appearance of organs
- I = Oedematous wall thickening
- II = Grade I + soft tissue infiltration
- III = Grade II + air bubbles in organ wall, free mediastinal or peritoneal air or fluid collection
- Grade II and III injuries are associated with an increased risk of strictures and oesophageal cancer.
Decontamination:
- The mouth may be rinsed with water as an immediate first aid measure
- Do not induce vomiting
- Do not administer oral fluids
- Do not administer activated charcoal
- Do not attempt pH neutralisation
Enhanced Elimination
- Not clinically useful.
Antidote
- None available.
Disposition
- Patients who are asymptomatic at 4 hours and tolerating oral fluids can be medically cleared.
- Symptomatic patients need to remain nil by mouth and are admitted for observation and further investigation within 24 hours. Management is then directed dependent on these findings.
- Patients with an airway compromise will require urgent intubation and ventilation with ongoing care on ICU.
- Patients with haemodynamic instability or evidence of perforation will require urgent surgical intervention and ICU admission.
Additional Resources and References:
Additional Resources:
- Tox conundrum 032 – Corrosive ingestion
- CCC – Corrosive ingestion
- Tox Flashcard – caustic ingestion acid and caustic ingestion alkali (below)

References:
- Lurie Y, Slotky M, Fischer D et al. The role of chest and abdominal computed tomography in assessing the severity of acute corrosive ingestion. Clinical Toxicology 2013; 51:834-837
- Munoz EM, et al. Massive necrosis of the gastrointestinal tract after ingestion of hydrochloric acid. European Journal of Surgery 2001:67: 195-198.
- Pelclová D, Navrátil T. Do corticosteroids prevent oesophageal stricture after corrosive ingestion? Toxicological Reviews 2005; 24(2):125-129.
- Zargar SA et al. Ingestion of corrosive alkalis. Spectrum of injury to upper gastrointestinal tract and natural history. American Journal of Gastroenterology 1992; 87(3):337-341

Toxicology Library
DRUGS and TOXICANTS
Dr Neil Long BMBS FACEM FRCEM FRCPC. Emergency Physician at Kelowna hospital, British Columbia. Loves the misery of alpine climbing and working in austere environments (namely tertiary trauma centres). Supporter of FOAMed, lifelong education and trying to find that elusive peak performance.