
![]()
CT Case 009
A 60yo female presents with 2 weeks of dyspnoea, pleuritic chest pain and bilateral calf tenderness.
She is haemodynamically stable, but has oxygen saturation of 90% on room air.
She is worked up for possible pulmonary embolus. Wells score 3 -> her D-dimer is 6.6mg/L (ref <0.5mg/L).


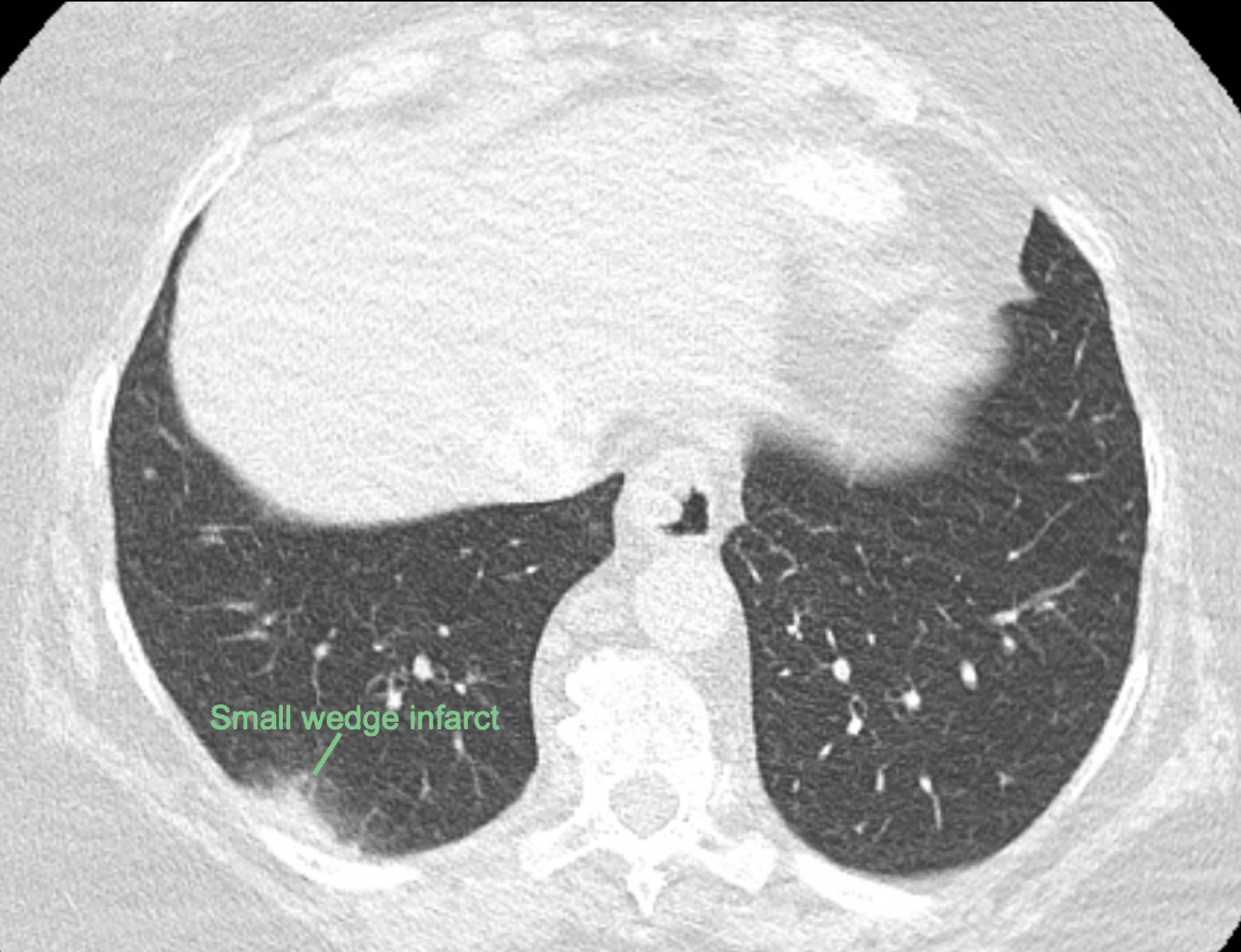
Describe and interpret the CT scan
CT INTERPRETATION
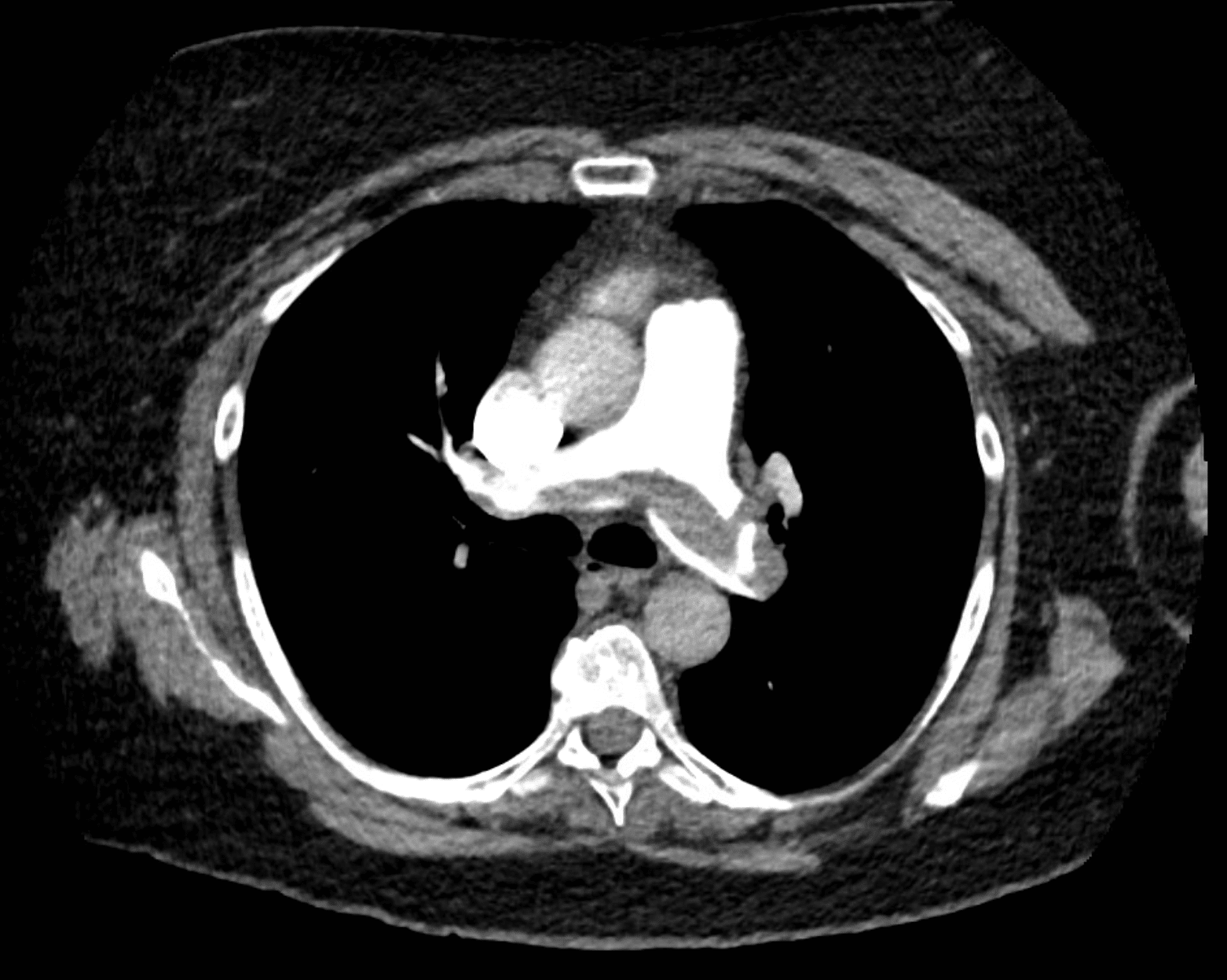
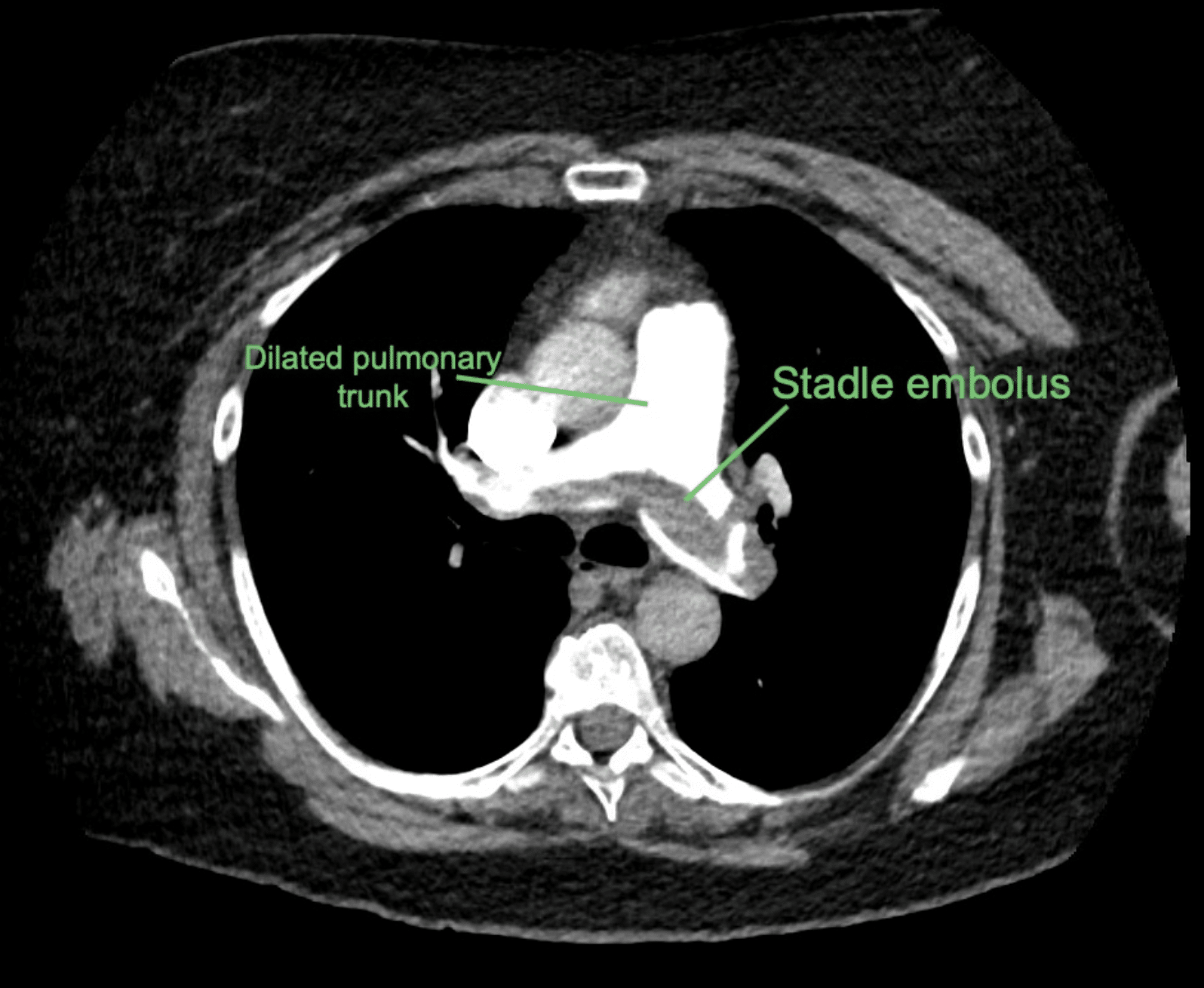
There is a saddle pulmonary embolism, with extension of embolus into the lobar and segmental branches of all lobes.
The right ventricle is dilated.
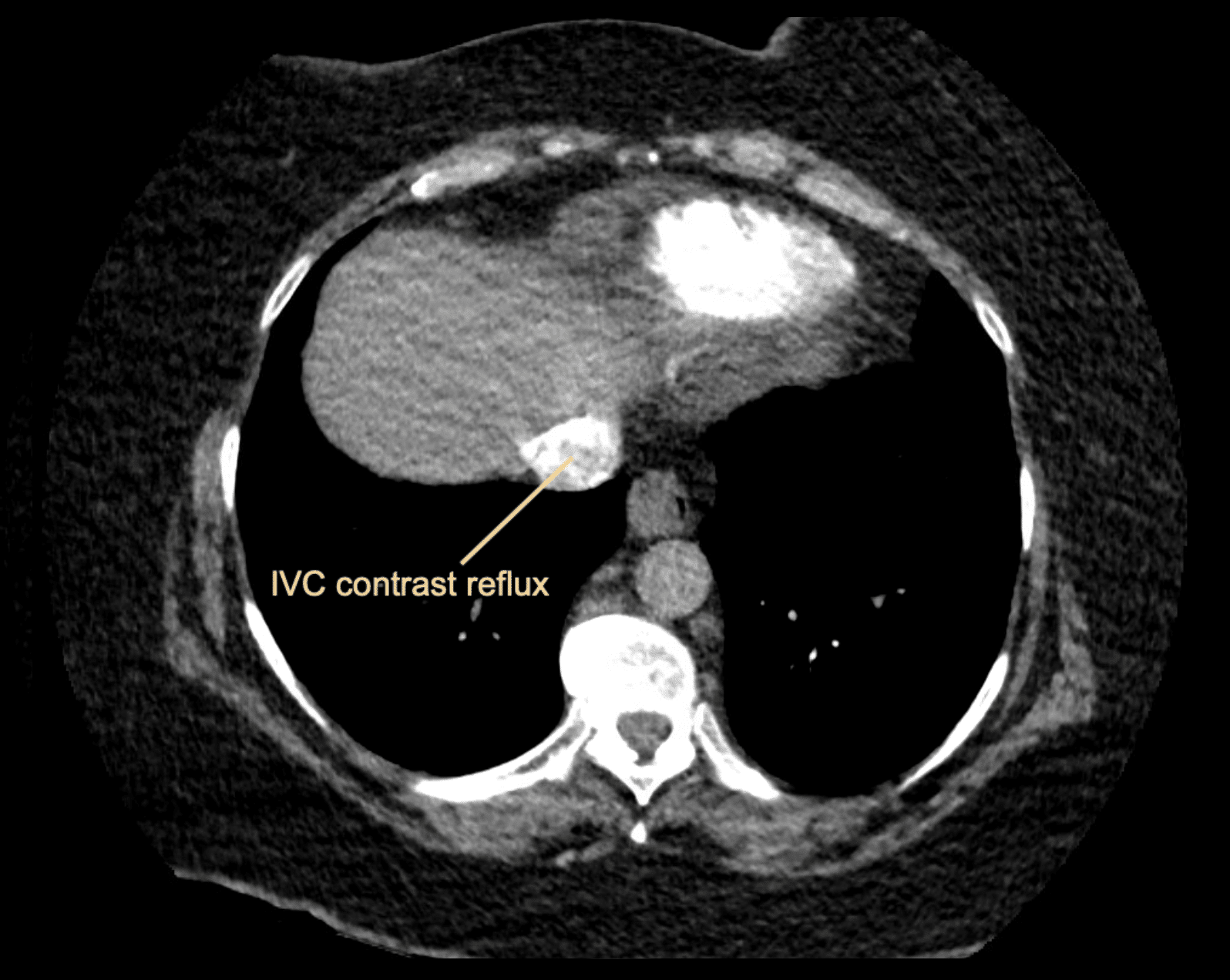
There is evidence of IV contrast reflux into the IVC. The pulmonary trunk is borderline dilated (at 29mm)
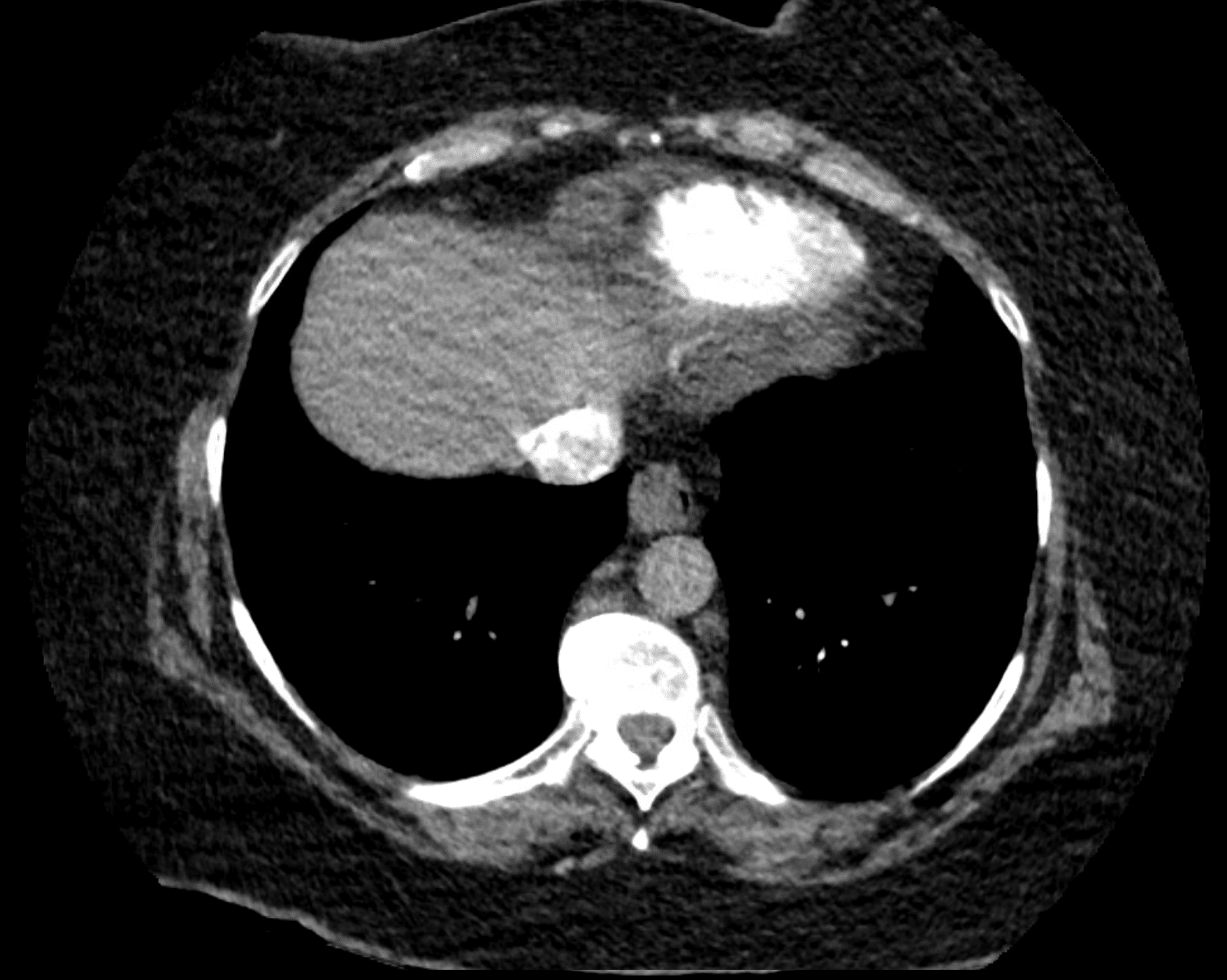
There is a small pulmonary infarct in the right base.

CLINICAL CORRELATION
This is a case of a submassive pulmonary embolism.
Submassive pulmonary embolus (PE) is an acute PE without systemic hypotension (SBP ≥90 mm Hg) but with either right ventricle (RV) dysfunction or myocardial necrosis.
The most obvious sign of right heart strain we see on this CT is the large right ventricle (RV). In a CT of a normal heart the RV is smaller than the left ventricle (LV), however here the RV:LV ratio is >1 consistent with right heart strain.
We also see flattening of the interventricular septum as the elevated right sided pressures cause it to be pushed into the left ventricle. In a normal heart we expect to see the septum bowing into the RV instead.
Other features of RHS we see on this CT are contrast reflux into the IVC. This also is due to elevated pulmonary pressures which push contrast media backwards into the IVC.
Lastly, the pulmonary artery is borderline dilated, also due to the high pulmonary pressures caused by the extensive clot burden.
Outcome
This patient was managed with a heparin infusion and eventually transitioned onto oral anticoagulation.
Lower limb doppler confirmed bilateral lower limb DVT.
Follow-up included serial monitoring of d-dimer, which can be used as a surrogate measurement of clot burden.
REFERENCES
- Nguyen PC, Stevens H, Peter K, McFadyen JD. Submassive Pulmonary Embolism: Current Perspectives and Future Directions. J Clin Med. 2021 Jul 30;10(15):3383.
- Wells’ Criteria for Pulmonary Embolism. MDcalc
- Nickson C. Pulmonary Embolism. CCC
- Burns E. ECG changes in Pulmonary Embolism ECG library
- Cadogan M. CXR eponyms in pulmonary embolism. LITFL
[cite]
TOP 100 CT SERIES

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney