![]()
CT Case 029
A 43 yo male presents with 5 days of cough, right sided chest pain and shortness of breath. He has a background of regular cannabis use (via a bong) and had a right sided pneumothorax four months prior.
He has mild signs of increased work of breathing and sats of 88%.
He was initially investigated with a CXR.
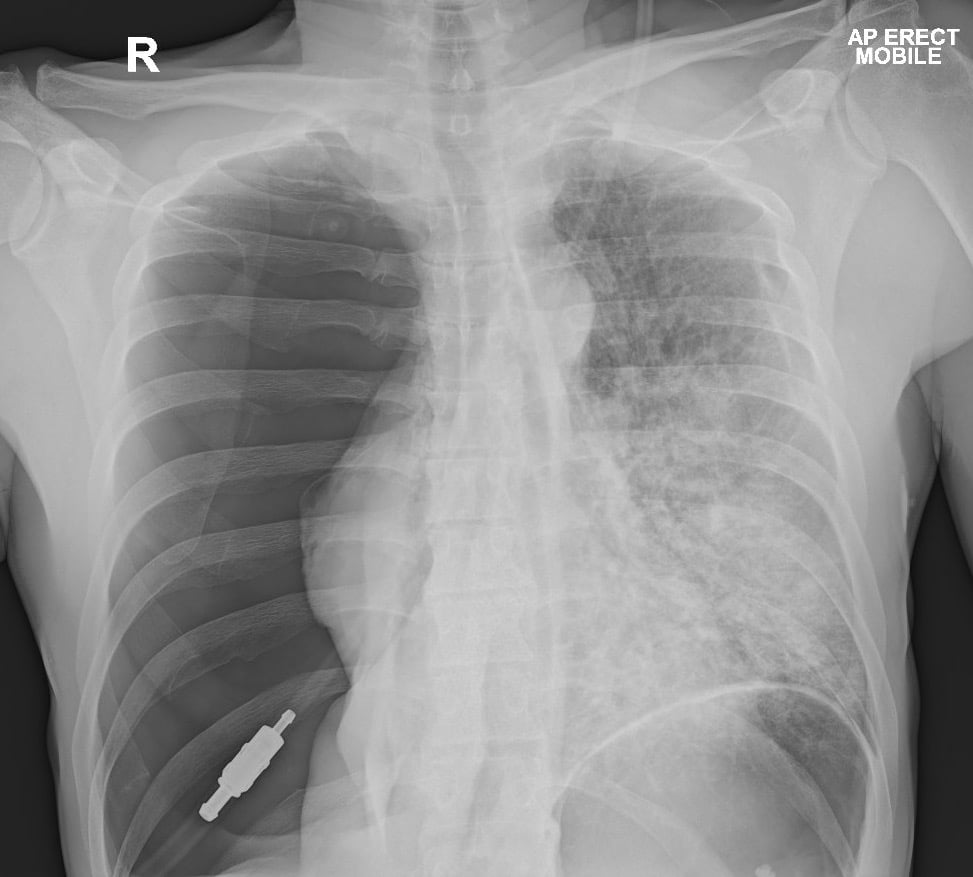
Describe and interpret the CXR
CXR INTERPRETATION
There is a large right sided pneumothorax (taking up the entire right hemithorax).
There are radiological features of tension, namely;
- mediastinum displaced to the left
- right hemidiaphragm is depressed
- increased rib spacing on the right
Normally such patients would present with severe respiratory distress and haemodynamic instability.
This patient only had mild symptoms, suggesting an acute on chronic presentation.
A pigtail catheter was inserted and the next day a CT chest was performed for further investigation of recurrent pneumothorax.

A pigtail catheter was inserted and the next day a CT chest was performed for further investigation of recurrent pneumothorax.
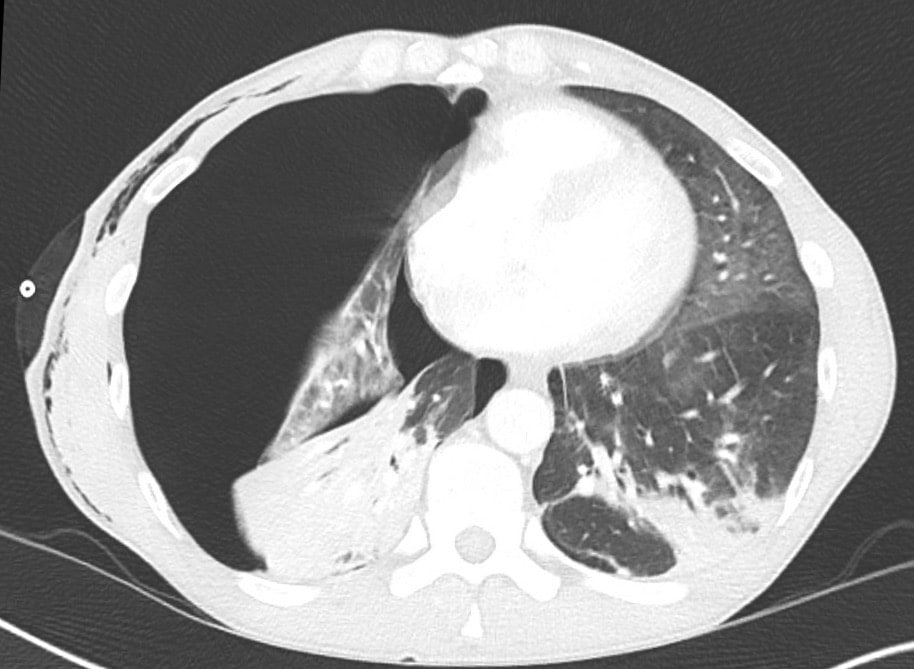


Describe and interpret the CT images
CT INTERPRETATION
There is persistent right sided pneumothorax (only partially resolved compared to the CXR pre-pigtail catheter insertion).
The mediastinum is still slightly displaced to the left.
There is subcutaneous emphysema along the right thoracic wall.
The CT confirmed correct catheter position without kinking of the catheter.
There is upper lobe para-septal emphysema (smoking related lung disease).
There are also patchy areas of consolidation in both left and right lungs.



CLINICAL CORRELATION
The combination of emphysematous changes in the lung as well as prolonged high-pressure breath holding manoeuvres during marijuana inhalation puts marijuana smokers at high risk of barotrauma -> resulting in pneumothorax, pneumomediastinum and subcutaneous emphysema.
Bong or pipe use also puts patients at risk of atypical infections (such as pseudomonas and aspergillus).
Outcome
This patient was treated with antibiotics for an atypical pneumonia. His lung eventually did re-expand although was slow to do so. The persistent collapse is likely present due to a combination of the underlying pneumonia as well as chronic collapse from recurrent pneumothorax.
If we see a persistent pneumothorax there are a few critical causes that need to be considered;
- Misplaced catheter
- Kinked catheter
- Bronchopleural fistula (very important cause to exclude – clinically this will be apparent due to persistent air leak despite correct catheter placement)
References
- Brims F. Tension pneumothorax – time to change the old mantra? LITFL
- Johnston M. Searching for Smaug. LITFL
- Brims F. Tension Pneumothorax – an alternative view. LITFL
- Own the Chest Tube. CCC
- Rippey J. Lung ultrasound: Pneumothorax. LITFL
- Nickson C. Pneumothorax. CCC
[cite]
TOP 100 CT SERIES

Emergency Medicine Education Fellow at Liverpool Hospital NSW. MBBS (Hons) Monash University. Interests in indigenous health and medical education. When not in the emergency department, can most likely be found running up some mountain training for the next ultramarathon.

Dr Leon Lam FRANZCR MBBS BSci(Med). Clinical Radiologist and Senior Staff Specialist at Liverpool Hospital, Sydney

Sydney-based Emergency Physician (MBBS, FACEM) working at Liverpool Hospital. Passionate about education, trainees and travel. Special interests include radiology, orthopaedics and trauma. Creator of the Sydney Emergency XRay interpretation day (SEXI).

Provisional fellow in emergency radiology, Liverpool hospital, Sydney. Other areas of interest include paediatric and cardiac imaging.