
![]()
Searching for Smaug
My armour is like tenfold shields, my teeth are swords, my claws spears, the shock of my tail is a thunderbolt, my wings a hurricane, and my breath death!
Smaug, the most powerful, the most cunning, and some would even say the greatest, dragon of the Third Age, had a story steeped in mystery. By the time an unexpected journey began, Smaug had not been seen for 150 years, but legend had it that he had laid waste to the Lonely Mountain in Erebor, and was feared as a ruthless killer.
The obvious questions that ensue from this frightening tale are:
- Does Smaug really exist, or is he some terrifying myth?
- If he does exist, is he a swift and definitive killer, feared by man, dwarf and elven folk alike?
- Does he have a weak spot, which is amenable to piercing by a single needle-like arrow, to smote him still and dead?
Just for a moment, as we take the Middle out of Earth, we consider the dragon of the current age.
The spontaneous tension pneumothorax
We shall look at the 3 questions posed.
Firstly – does it exist, or is it some terrifying myth?
We have all had the experience of the tension phenomena in the setting of trauma, or in the iatrogenic setting, particularly in conjunction with positive pressure ventilation.
There are some that would say that the occurrence of a primary spontaneous tension pneumothorax in a spontaneously ventilating patient is incredibly rare. There are very few reported cases in the literature
- Spontaneous Pneumothorax: Is it under tension? [J Accid Emerg Med 2000]
- Spontaneous Tension Pneumothorax. [NEJM 2010]
This post arose from 2 curious happenstances.
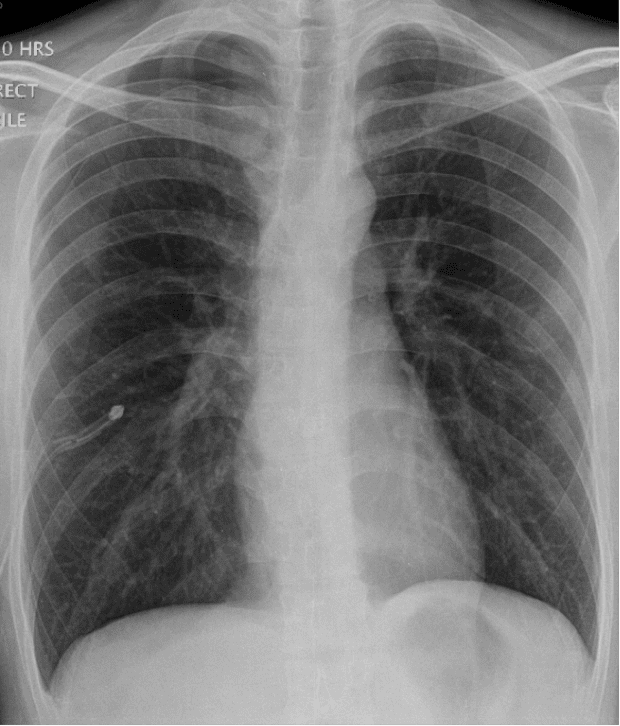
The first was a clinical case of a young man, a non-smoker, a non-partaker of illicit substances. He presented to ED several hours after the onset of right pleuritic chest pain and shortness of breath. His observations showed a persistent and worsening tachycardia and developing hypotension. At the time of his CXR he had a HR of 125 and a systolic BP of 90mmHg. Sao2 on air were 93%.
View the original CXR

Is this a tension? Not much mediastinal shift on the CXR I hear you say. But what about the tachycardia and hypotension? Blunt tools I admit, but pretty impressive in a young fit man.
So, we did something a little crazy. Whilst preparing to put in a narrow bore intercostal catheter, we put a needle into the 5th ICS AAL and hooked him up to the invasive pressure monitor, to see if we could answer the question! The monitor showed a very steady 17mmHg, with only minor fluctuations with the respiratory cycle. What does this mean? We don’t know, as there is next to no literature about this. Several animal studies have looked at intrapleural pressures in induced porcine pneumothoraces, whereby discreet volumes of air are induced (apparently the swine model most closely resembles the human condition, because the intact mediastinal pleura is similar, but this seems a long bow) – (and I haven’t seen mentioned made of a dragon model). At 0, 10 , 20 cmH20 increases in intrapleural pressures, there is little change in SVC, oesophageal and CO pressures/parameters, but at 10 and 20 cm H20 the HR starts to increase.
- The Pathophysiology of tension pneumothorax in ventilated swine. [J Emerg Med. 1997]
We plan to look out for further cases to see how reproducible this is (and perhaps put the call out to FOAMites to consider doing the same – to consider transducing a pressure from a needle inserted at the time of preparing to drain a PTx)
As soon as his ICC was placed, his HR dropped to <90, and his SBP went up to >110mmHg.
Post procedure CXR
The other unhappy circumstance that led to this post was a case of which I became peripherally aware, in the prehospital setting, whereby the adherence to an algorithm in a patient who had an out of hospital PEA arrest, led to a series of events whereby a patient had bilateral needle thoracostomies performed. The patient recovered from their PEA arrest, which was probably, in retrospect, anaphylactic in nature. They then, however, expired from a massive haemothorax, probably as a result of a needle thoracostomy.
It is not appropriate to dive into the details of this case, but it does serve to illustrate a case for reviewing a risk: benefit analysis. If primary spontaneous pneumothorax is incredibly rare, are we well served by seeking it out so aggressively?
Thus to ponder the second question.
Is a primary spontaneous tension pneumothorax a ruthless, swift and silent killer, or is it, in fact, urban legend, dogma passed down through the ages like tales around a flickering fire in the dark?
The third question leaves us on far more solid ground.
Smaug slumbered for centuries on his plundered treasure, allowing his soft and vulnerable underbelly to be impregnated with gold and gems, protecting him from attack, where his scales finished. The nominated ‘burglar’, one Bilbo Baggins, discovered a single bare patch over Smaug’s left breast, whilst pilfering a small gold goblet. This information was leaked, allowing Smaug to meet his demise at the hands of a single man, wielding a needle-like arrow, which pierced this very spot.
Even if we do believe that the primary spontaneous tension pneumothorax exists, does a lone angiocath, plunged deep into the flesh of the 2nd ICS MCL redeem the situation?
The needle is too short, kinks too freely, and has unclear endpoints. For references for this, I direct you, once again, to the Kings and Queens of the FOAM realms, who have published much, and referred to the original evidence.
- EMCrit – Needle Finger thoracostomy
- Academic Life in Emergency Medicine – Don’t miss the pneumothorax
- Resus Me – Needle decompression – it’s still not going to work
So what do we know?
Thus, we are left with few definitive and certain points.
There have been documented cases of primary spontaneous tension pneumothorax.
The case that I have brought before you is undefined. It is certainly not clear whether this was truly a tension – although he had clear cardiovascular (albeit mild) compromise, his CXR changes were unexciting, and his measured intrapleural pressures were undecipherable in the face of a lack of comparable evidence.
Needle thoracostomy is a procedure, steeped in dogma, but without much proven benefit, and high potential risks, in this subset of patients. There is no question that its utility ought to be severely questioned if following an algorithmic course for management of PEA arrest.
If you have any experience, either with primary spontaneous tension pneumothoraces, or indeed, with dragon-slaying, I would encourage you to share them in this new FOAMed realm. Perhaps we can achieve what literature, both fiction, and non- has been unable to do, and definitively answer this question.
LITFL Further Reading
- Brims F. Tension pneumothorax – time to change the old mantra? LITFL
- Johnston M. Searching for Smaug. LITFL
- Brims F. Tension Pneumothorax – an alternative view. LITFL
- Own the Chest Tube. CCC
- Rippey J. Lung ultrasound: Pneumothorax. LITFL
- Nickson C. Pneumothorax. CCC
- Top 100 CXR
[cite]

Critical Care
Compendium
Emergency physician. Lives for teaching and loves clinical work, but with social media, she is like the syndromic cousin in the corner who gets brought out and patted on the head once in a while | Literary Medicine | @eleytherius | Website |