
![]()
Dangerous Love
Love can be dangerous.
No, I’m not talking about revenge killings by jilted lovers, sexually transmitted infections, or the intrinsic hazards of extramarital dalliances. Love itself is dangerous. If you don’t believe me, read on to learn about all the ways amorous acts can threaten life, limb and… other body parts.
Overview
The neglect of this topic in emergency medicine training seems a gross oversight. For a quick overview, a good place to start is a paper titled ‘Coital Emergencies’. Banerjee highlights a number of ‘common’ coital emergencies (though, strangely, he seems to neglect female genital injury):
- Neurological — benign coital headache, aneurysmal subarachnoid haemorrhage, cerebrovascular accidents
- Urological — penile fracture, priapism, preputial tears, penile vessel rupture
- Cardiovascular — sudden cardiac death, myocardial infarction
- Soft tissue — soft tissue wounds, soft tissue infection
- Immunological — local allergic reactions, anaphylaxis
- Banerjee A. Coital emergencies. Postgrad Med J. 1996 Nov;72(853):653-6.
Risk of sex death
Data on the risk of death during intercourse aren’t great. One retrospective study found that of people that die, about 1 in 500 were having intercourse at the time (or thereabouts). One suspects the rate could be higher: do you routinely asks the bereaved, “So, were you having sex at the time?”? The cause of death during intercourse is usually myocardial infarction, although intracerebral hemorrhage and subarachnoid hemorrhage must not be forgotten.
- Parzeller M, Raschka C, Bratzke H. Sudden cardiovascular death in correlation with sexual activity — results of a medicolegal postmortem study from 1972–1998. Eur Heart J. 2001 Apr;22(7):610-1. PMID: 11259149.
- Reynolds MR, Willie JT, Zipfel GJ, Dacey RG. Sexual intercourse and cerebral aneurysmal rupture: potential mechanisms and precipitants. J Neurosurg. 2010 Jun 11. PMID: 20540599.
So far, so good. What we’ve discussed so far has been fairly standard. But seriously weird and bad things can happen during acts of love… As you’re about to find out.
Love bites
A recent report from New Zealand described a case of partial paralysis due to a ‘hickey’ or ‘love bite’. Excess suction was applied over her internal carotid artery, resulting in thrombosis…
Two views of the internal carotid artery in the affected patient. The arrows point to thrombus. Longitudinal view on the left, transverse on the right. From Wu et al (2010) (Click image for source)
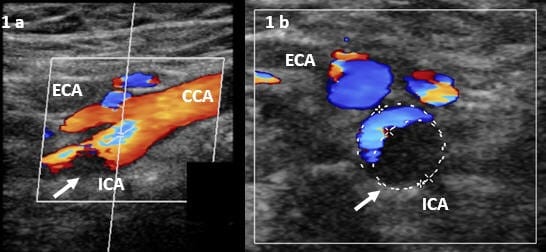
- Wu TY, Hsiao J, Wong EH. Love bites — an unusual cause of blunt internal carotid artery injury.NZMJ. 2010; 123(1326) PMID: 21326406 [full text]
Love allergies
Allergies and love do not mix. Steensma has described how a good night kiss, from a shrimp-eating boyfriend, nearly killed his shellfish-allergic girlfriend. Furthermore, women can actually be allergic to sex. Acute systemic hypersensitivity or localised vulvovaginitis can occur as a result of allergic reactions to semen. The sensitivity is not partner specific — condoms or abstinence are the immediate options for cure. Also, exogenous allergens (such as Brazil nuts, for example) can find their way into semen, and cause allergic reactions in receptive partners. Finally, there is an odd condition that can affect men (@DrVes told me about it) known as Postorgasmic illness syndrome (POIS). POIS is a combination of local allergic symptoms and transient flu-like illness. It may be that POIS is triggered by ejaculation and results from hypersensitivity to the male’s own semen!
- Allergy Notes: Sexually transmitted allergy to Brazil nuts. [link]
- Jones WR. Allergy to coitus. Aust N Z J Obstet Gynaecol. 1991 May;31(2):137-41. PMID: 1681800.
- Steensma DP. The kiss of death: a severe allergic reaction to a shellfish induced by a good-night kiss. Mayo Clin Proc. 2003 Feb;78(2):221-2. PMID: 12583533.
- Waldinger MD, Meinardi MM, Zwinderman AH, Schweitzer DH. Postorgasmic Illness Syndrome (POIS) in 45 Dutch Caucasian Males: Clinical Characteristics and Evidence for an Immunogenic Pathogenesis (Part 1). J Sex Med. 2011 Jan 17. [Epub ahead of print] PMID: 21241453.
Love emboli
Air emboli from sex can kill. The risk is probably higher not long after birth (especially if amphetamines are taken prior to intercourse), as it may take a while for those big uteroplacental arteries to involute after birth. However, vaginal tears from consensual intercourse, irrespective of pregnancy status, also have the potential to cause fatal air emboli. As always, any paper written by Batman is a must read:
- Batman PA, Thomlinson J, Moore VC, Sykes R. Death due to air embolism during sexual intercourse in the puerperium. Postgrad Med J. 1998 Oct;74(876):612-3. PMC2361003.
- Moreschi C, Da Broi U. Paradoxical air embolism through patent foramen ovale during consensual intercourse in a non-pregnant young female. J Forensic Leg Med. 2009 Nov;16(8):482-5. PMID: 19782322.
Traumatic love and its complications
Vaginal injuries from consensual intercourse can lead to other problems. Pneumoperitoneum was reported following ‘conventional’ intercourse, with a 4cm vaginal laceration identified as the culprit. There was no mention of whether genital jewelry was involved. Another nasty complication from ‘normal’ coitus, as described by Ijaiya et al (2009) is rectovaginal fistula formation. The victim was later divorced by her loving husband.
- Manchanda R, Refaie A. Acute pneumoperitoneum following coitus. CJEM. 2005 Jan;7(1):51-3. PMID: 17355655.
- Ijaiya MA, Mai AM, Aboyeji AP, Kumanda V, Abiodun MO, Raji HO. Rectovaginal fistula following sexual intercourse: a case report. Ann Afr Med. 2009 Jan-Mar;8(1):59-60. PMID: 19763010.
Penis injuries are a bit ho-hum for the seasoned emergency physician. But, it is probably worth mentioning posterior urethral injury as a cause of hematospermia after intercourse and to provide a link to a nasty case of penile fracture associated with urtheral injury. Some blokes need target practice… or less acrobatic partners.
- Boncher NA, Vricella GJ, Jankowski JT, Ponsky LE, Cherullo EE. Penile fracture with associated urethral rupture. Case Report Med. 2010;2010:791948. PMID: 21076536; PMCID: PMC2975082.
- Cheng YS, Lin JS, Lin YM. Isolated posterior urethral injury: an unusual complication and presentation following male coital trauma. Asian J Androl. 2006 May;8(3):379-81. PMID: 16625291.
The mystery of penis captivus
Finally, we wouldn’t be living in the fast lane if we didn’t mention the most enigmatic of all coital conditions, penis captivus. Here are some relative modern reports from the BMJ suggesting that, yes, the condition actually does exist.
- Taylor FK. Penis captivus — did it occur? Br Med J. 1979 Oct 20;2(6196):977-8.
- Musgrave B. Penis captivus has occurred. Br Med J. 1980 Jan 5;280(6206):51. PMC1600543.
I have a high degree of suspicion regarding the spuriosity of the cases in Taylor’s review. One in particular stands out:
“Kisch, in his Sexual Life of Women,- speaks of “more or less credible instances of penis captivus” being on record. He mentions an account by a medical man called Davis, not otherwise identified, who was one day called to a couple found in this “most compromising position. All the endeavours of the pair thus surprised to separate proved ineffectual, and their attempts to draw apart caused them intense pain. Davis… ordered an iced douche, which, however, failed to liberate the imprisoned penis. Release was impossible until the woman had been placed under chloroform. The swollen and livid penis exhibited two strangulation-furrows.””
A medical man called Davis? Who could that be I wonder? Perhaps an ancestor of UCEM’s PR Supervisor, the famed psychiatric surgeon Assistant Sub-Professor Egerton Y. Davis IV? Surely not? Read penis captivus and decide for yourself… As for the letter by Musgrave, one cannot help but wonder about medical doctors and their overactive imaginations. Indeed, the BMJ was clearly having a good month for letters back then — the letter immediately preceding it concerned ‘The Interesting New Zealander‘.
Conclusion
Life is a risky business. It is for the individual to decide if how they live it is worth the risk. But, what would life be without love?
Safer, is one answer.
Chris is an Intensivist and ECMO specialist at The Alfred ICU, where he is Deputy Director (Education). He is a Clinical Adjunct Associate Professor at Monash University, the Lead for the Clinician Educator Incubator programme, and a CICM First Part Examiner.
He is an internationally recognised Clinician Educator with a passion for helping clinicians learn and for improving the clinical performance of individuals and collectives. He was one of the founders of the FOAM movement (Free Open-Access Medical education) has been recognised for his contributions to education with awards from ANZICS, ANZAHPE, and ACEM.
His one great achievement is being the father of three amazing children.
On Bluesky, he is @precordialthump.bsky.social and on the site that Elon has screwed up, he is @precordialthump.
| INTENSIVE | RAGE | Resuscitology | SMACC