
![]()
ECG Case 099
ECG from a 19 yr old referred by their GP for investigation of palpitations found at a routine medical review. The patient is asymptomatic with no past medical history or regular medications.

Describe and interpret this ECG
ECG ANSWER and INTERPRETATION
Rate:
- Mean ventricular rate 60 bpm
Rhythm:
- Complicated and difficult to fully ascertain on a single ECG
- Atrial activity seen
- P waves clearly visible
- Variable P-P interval
- Represents ventriculophasic sinus arrhythmia
- Apparent drop of P waves before 2nd, 3rd, and 4th ventricular ectopics
- I think the P waves are actually buried in the initial portion of the wide QRS best appreciated in the 4th ventricular ectopic (green circle) rather than representing SA exit block.

- Evidence of AV block
- Multiple non-conducted P waves
- No progressive PR prolongation evident – longer rhythm strip would be helpful
- 2nd Degree AV Block Mobitz II
- Frequent PVC’s
- 4 During 10 second recording
- Likely unifocal
- 1st PVC likely has some fusion due to proximity to preceding P wave
Axis (Conducted QRS):
- Normal
Intervals (Conducted QRS):
- PR – Prolonged (220ms)
- QRS – Normal
- QT – 340ms
CLINICAL PEARLS
The ECG in Athlete’s
There are a number of adaptive physiological changes seen in athlete’s as a response to regular exercise including cardiac changes such as change in LV wall thickness or end-diastolic LV volume (Lisman KA). These physiological adaptations can also be manifest as changes on the 12-lead ECG.
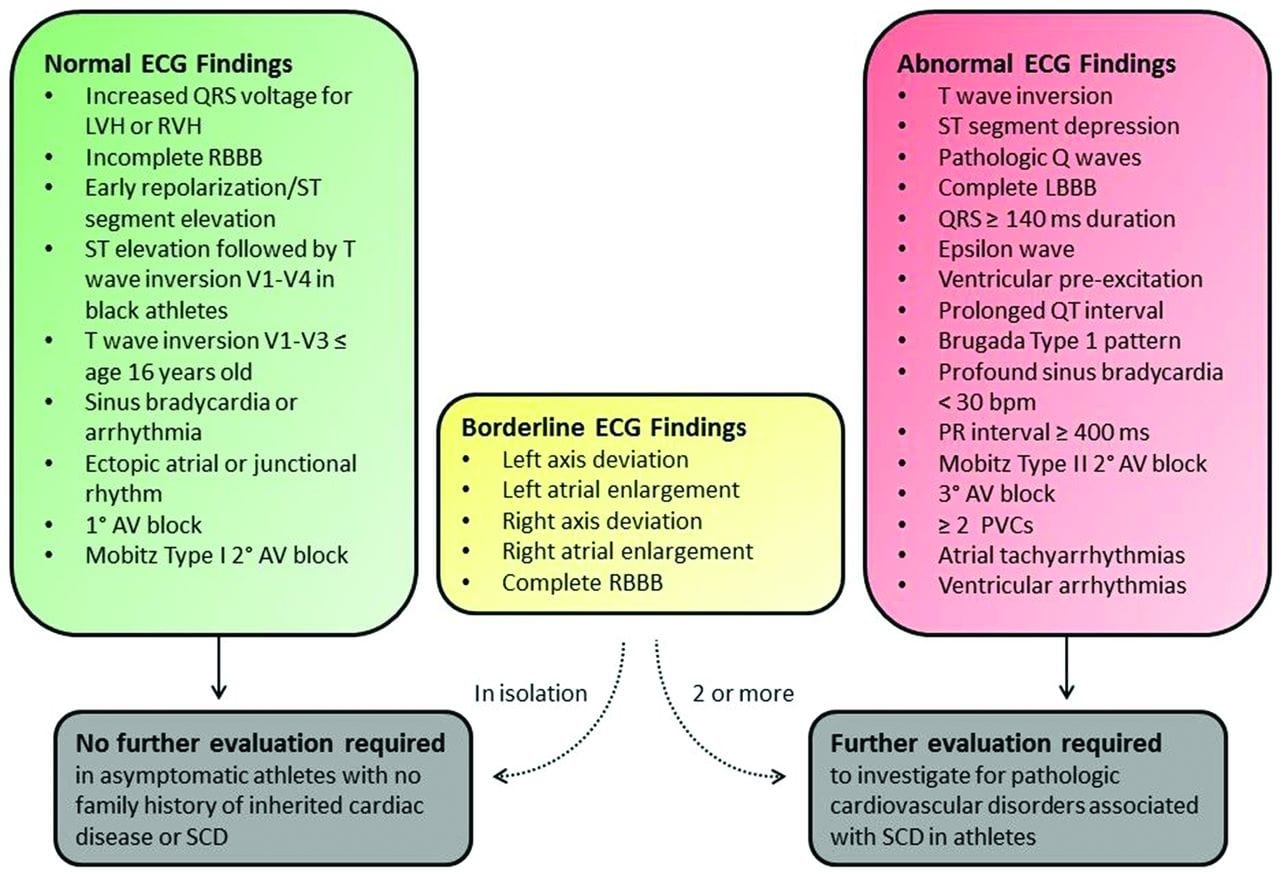
The challenge for clinicians is picking those changes that require further investigation for potential causes of sudden cardiac death versus those that represent normal adaptation.Thankfully there is an Consensus International Criteria for ECG Interpretation in Athletes, aka ‘Seattle criteria’, developed in 2015 with the latest version published in BJSM in 2017.
It provides guidance on those ECG features that can be considered a normal response to exercise, those that are ‘borderline’ and those that require further investigation. The updated version also provided guidance on differentials associated with each ECG abnormality and appropriate investigation modalities. The following flow chart summaries these groups of ECG findings:
CASE OUTCOME
In Our Case
The abnormal findings seen on this ECG:
- Frequent PVC’s – 4 seen in 10 second window equating to up to ~35000/day
- Mobitz II AV Block
Differential causes for these features include:
- Arrhythmogenic Right Ventricular Cardiomyopathy – can genetic or induced
- Left Ventricular Non-Compaction
- Dilated Cardiomyopathy
- Hypertrophic Cardiomyopathy
- Sarcoidosis
- Myocarditis
Refer patient for further cardiac investigation which may include echo, 24-holter, ILR, EP study and cardiac MRI
REFERENCES
- Drezner JA, Sharma S, Baggish A, et al. International criteria for electrocardiographic interpretation in athletes: Consensus statement. Br J Sports Med 2017;51:704-731
- Drezner JA, Ackerman MJ, Cannon BC, et al. Abnormal electrocardiographic findings in athletes: recognising changes suggestive of primary electrical disease. Br J Sports Med 2013;47:153-167.
- Drezner JA, Ashley E, Baggish AL, et al. Abnormal electrocardiographic findings in athletes: recognising changes suggestive of cardiomyopathy. Br J Sports Med 2013;47:137-152.
- Lisman KA. Electrocardiographic Evaluation in Athletes and Use of the Seattle Criteria to Improve Specificity. Methodist DeBakey Cardiovascular Journal. 2016;12(2):81-85.
TOP 100 ECG Series
Emergency Medicine Specialist MBChB FRCEM FACEM. Medical Education, Cardiology and Web Based Resources | @jjlarkin78 | LinkedIn |

dont you think that the ventricular complexes are ventricular escape beats
I think there are definite Wenckebach periods (beats 4, 5 and 7, 8, each followed by a nonconducted P). There are escape beats (2, 3 for example) that I would guess are juctional in origin. Beat 2 is preceded by a P but with a short PR. The escape beat got to the ventricle first.
yes me thinking same these r ventriclar escape beats
There is no PVC (not prematured) but ventricular escape beats… bloc AV with thin QRS are mostly Mobitz I block