
![]()
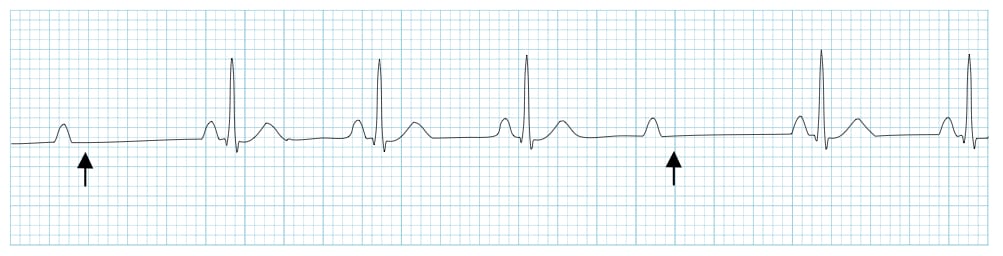
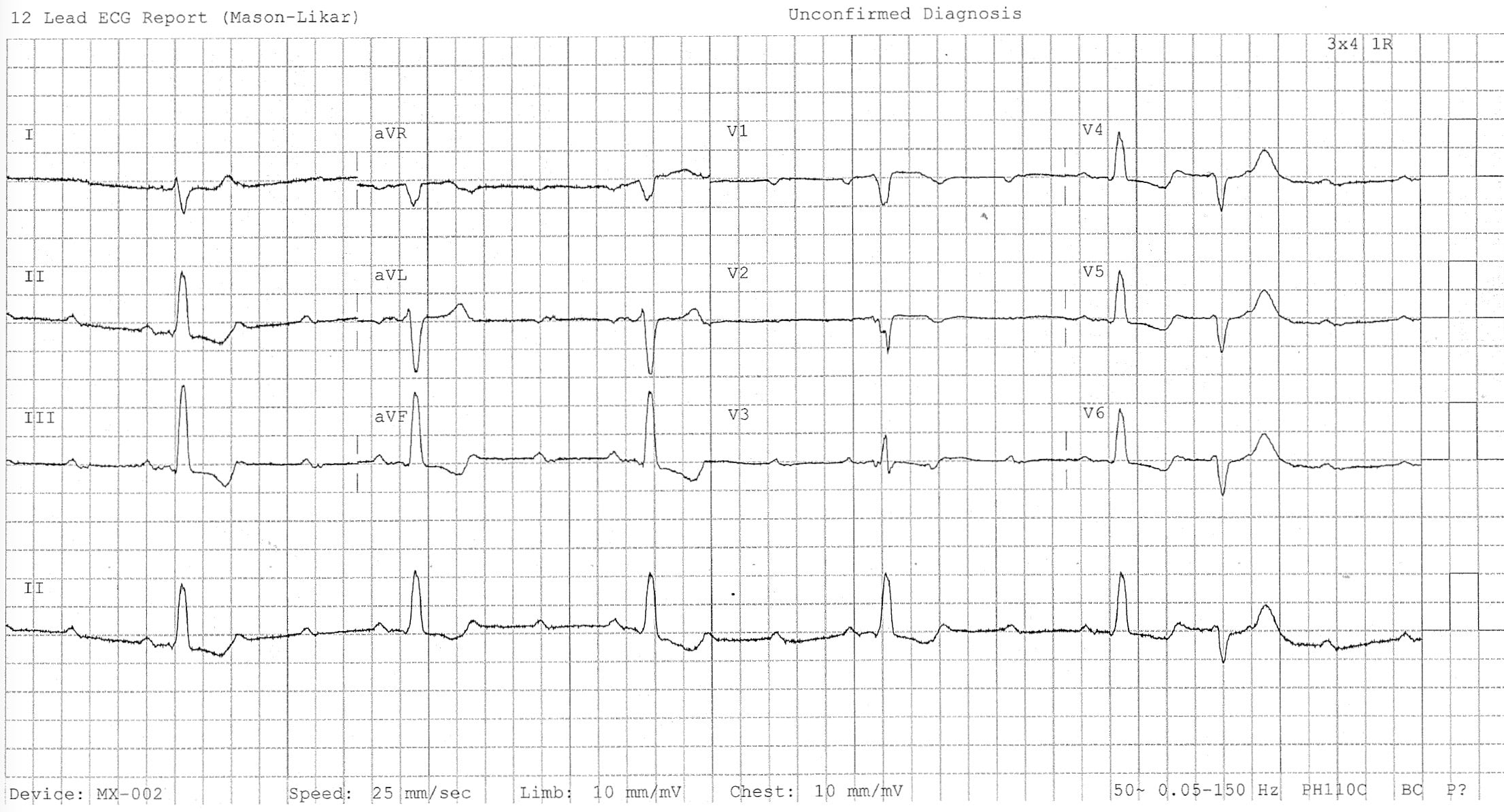
AV Block: 2nd degree, Mobitz II (Hay block)
Definition of Mobitz II block (Hay Block)
A form of 2nd degree AV block in which there is intermittent non-conducted P waves without progressive prolongation of the PR interval
Other features:
- The PR interval in the conducted beats remains constant
- The P waves ‘march through’ at a constant rate
- The RR interval surrounding the dropped beat(s) is an exact multiple of the preceding RR interval (e.g. double the preceding RR interval for a single dropped beat, triple for two dropped beats, etc)

Mechanism
- Mobitz II is usually due to failure of conduction at the level of the His-Purkinje system (i.e. below the AV node)
- While Mobitz I is usually due to a functional suppression of AV conduction (e.g. due to drugs, reversible ischaemia), Mobitz II is more likely to be due to structural damage to the conducting system (e.g. infarction, fibrosis, necrosis)
- Patients typically have a pre-existing LBBB or bifascicular block, and the 2nd degree AV block is produced by intermittent failure of the remaining fascicle (“bilateral bundle-branch block”)
- In around 75% of cases, the conduction block is located distal to the Bundle of His, producing broad QRS complexes.
- In the remaining 25% of cases, the conduction block is located within the His Bundle itself, producing narrow QRS complexes.
- Unlike Mobitz I, which is produced by progressive fatigue of the AV nodal cells, Mobitz II is an “all or nothing” phenomenon whereby the His-Purkinje cells suddenly and unexpectedly fail to conduct a supraventricular impulse.
- There may be no pattern to the conduction blockade, or alternatively there may be a fixed relationship between the P waves and QRS complexes, e.g. 2:1 block, 3:1 block.
Causes of Mobitz II
- Anterior MI (due to septal infarction with necrosis of the bundle branches)
- Idiopathic fibrosis of the conducting system (Lenègre-Lev disease)
- Cardiac surgery, especially surgery occurring close to the septum e.g. mitral valve repair
- Inflammatory conditions (rheumatic fever, myocarditis, Lyme disease)
- Autoimmune (SLE, systemic sclerosis)
- Infiltrative myocardial disease (amyloidosis, haemochromatosis, sarcoidosis)
- Hyperkalaemia
- Drugs: beta-blockers, calcium channel blockers, digoxin, amiodarone
Clinical Significance
- Mobitz II is much more likely than Mobitz I to be associated with haemodynamic compromise, severe bradycardia and progression to 3rd degree heart block
- Onset of haemodynamic instability may be sudden and unexpected, causing syncope (Stokes-Adams attacks) or sudden cardiac death
- The risk of asystole is around 35% per year
- Mobitz II mandates immediate admission for cardiac monitoring, backup temporary pacing and ultimately insertion of a permanent pacemaker
Examples
ECG 1
Related Topics
- AV block: 1st degree
- AV block: 2nd degree, Mobitz I
- AV block: 2nd degree, “fixed ratio blocks” (2:1, 3:1)
- AV block: 2nd degree, “high grade AV block”
- AV block: 3rd degree (complete heart block)
- Eponymythology: History of Second-degree AV block. 2020
- Eponym: Karel Frederik Wenckebach (1864 -1940). LITFL 2020
- Eponym: Woldemar Mobitz (1889 – 1951). LITFL 2020
- Eponym: John Hay (1873 – 1959). LITFL 2020
Advanced Reading
Online
- Wiesbauer F, Kühn P. ECG Mastery: Yellow Belt online course. Understand ECG basics. Medmastery
- Wiesbauer F, Kühn P. ECG Mastery: Blue Belt online course: Become an ECG expert. Medmastery
- Kühn P, Houghton A. ECG Mastery: Black Belt Workshop. Advanced ECG interpretation. Medmastery
- Rawshani A. Clinical ECG Interpretation ECG Waves
- Smith SW. Dr Smith’s ECG blog.
- Wiesbauer F. Little Black Book of ECG Secrets. Medmastery PDF
Textbooks
- Zimmerman FH. ECG Core Curriculum. 2023
- Mattu A, Berberian J, Brady WJ. Emergency ECGs: Case-Based Review and Interpretations, 2022
- Straus DG, Schocken DD. Marriott’s Practical Electrocardiography 13e, 2021
- Brady WJ, Lipinski MJ et al. Electrocardiogram in Clinical Medicine. 1e, 2020
- Mattu A, Tabas JA, Brady WJ. Electrocardiography in Emergency, Acute, and Critical Care. 2e, 2019
- Hampton J, Adlam D. The ECG Made Practical 7e, 2019
- Kühn P, Lang C, Wiesbauer F. ECG Mastery: The Simplest Way to Learn the ECG. 2015
- Grauer K. ECG Pocket Brain (Expanded) 6e, 2014
- Surawicz B, Knilans T. Chou’s Electrocardiography in Clinical Practice: Adult and Pediatric 6e, 2008
- Chan TC. ECG in Emergency Medicine and Acute Care 1e, 2004
LITFL Further Reading
- ECG Library Basics – Waves, Intervals, Segments and Clinical Interpretation
- ECG A to Z by diagnosis – ECG interpretation in clinical context
- ECG Exigency and Cardiovascular Curveball – ECG Clinical Cases
- 100 ECG Quiz – Self-assessment tool for examination practice
- ECG Reference SITES and BOOKS – the best of the rest
ECG LIBRARY
Emergency Physician in Prehospital and Retrieval Medicine in Sydney, Australia. He has a passion for ECG interpretation and medical education | ECG Library |

MBBS FACEM DDU (Emergency) CCPU. Emergency Physician in Melbourne, Australia. Co-Ultrasound Lead for Emergency Medicine at The Alfred Hospital. Special interests in diagnostic and procedural ultrasound, medical education, and ECG interpretation. Editor of the LITFL ECG Library.

Thank you very much for your site! I’am a 25years-experience-old nurse and I have been an EMT for 11years in Montreal, Canada. I looooooove the quality and clarity of your descriptions of any cardiac rhythms I read about.
I’am currently working as a nursing educator. I recommand your site to ALL the young/old any nurses/lpn I worked with.